
 Indexed in Index Medicus and Medline
Indexed in Index Medicus and MedlineAn estimated 73,510 patients will be diagnosed with bladder cancer in the United States in 2012.1 Initial treatment of these tumors involves transurethral resection, however as many as 60%-70% of superficial urothelial carcinomas will recur.2 This may partly be due to the inability to detect some small papillary tumors and transitional carcinoma in situ (CIS) under standard white light cystoscopic conditions. A new technique to improve the visualization of tumors, combining an intravesical agent with a specific blue light cystoscopic system, was approved by the FDA in 2010.
Hexaminolevulinate HCl (HAL) is available in the United States as Cysview (Photocure US, Princeton, NJ, USA). In Europe it has been available for several years under the brand name of Hexvix. The product is designed to enhance the detection of non-muscle invasive bladder cancer (NMIBC). When instilled intravesically, it improves the visualization of bladder tumors through fluorescence cystoscopy with abnormal areas of the bladder fluorescing under blue light examination, hence the common name of “blue light” cystoscopy.
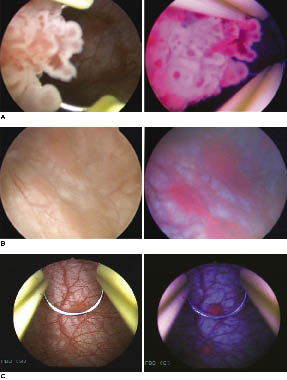
The intravesically administered compound is hexaminolevulinic acid, an ester that when applied topically will bypass cellular regulation mechanisms for heme synthesis and drive the accumulation of protoporphyrin IX (PpIX). PpIX fluoresces red with blue light and because PpIX accumulation preferentially occurs in malignant cells can be used to identify malignant tissue using HAL fluorescence cystoscopy (HAL-FC), Figure 1.3
Equipment
To incorporate HAL-FC into your clinical care for bladder cancer you will need “blue light” compatible cystoscopic instruments as well as facility Pharmacy committee approval for the Cysview. Currently the FDA has only approved the Karl Storz D-Light C Photodynamic Diagnostic (PDD) system (Karl Storz, Endoscopy-America, Inc. El Segundo, CA, USA). Our experience has been with using D-Light C light source in conjunction with the Tricam SL II and PDD camera head. The Storz AIDA HD connect system captures video and still images and images with this article were captured using this system, Figure 2a. The D-Light C light source contains a 300 Watt xenon arc lamp with a band pass filter capable of producing white and blue light (wavelength 360 nm-450 nm) which is carried to the telescope using a Storz fluid light cable. Specific Storz PDD telescopes are required (available with 0, 12, 30, and 70 degree viewing angles) that contain a filter that is necessary to detect fluorescence. They are 30 cm in length and are compatible with current Storz rigid cystoscopy sets, Figure 2b. Compatible flexible instruments are not available at this time.
The PDD camera has a blue and silver buttons that allow the operator to switch between blue and white light in addition to controlling gain, shutter speed, and white balancing. Understanding these controls can be useful to the surgeon to optimize image quality. Pressing the blue button for 1 sec will switch in between blue and white light while pressing the blue button for > 3 sec will white balance the camera. The silver button will control shutter speed in either blue or white light mode. Default shutter speed is 1/15 second and can be changed by holding the silver button > 3 sec. While using blue light a shutter speed of 1/15 or 1/30 second is recommended. A 1 sec press of the silver button will allow the operator to cycle through gain settings to adjust lamp brightness during use.4
Patient selection
Cysview is approved for one-time use in patients with known or suspected non-muscle invasive bladder cancer and only for use with the Karl Storz D-Light C Photodynamic Diagnostic (PDD) system. It is contraindicated in patients with porphyria, gross hematuria, BCG treatment within 90 days, or known hypersensitivity to Cysview or other 5-ALA derivative.5
We have found clinical utility in HAL-FC consistent with recommendations recently published by a European panel of experts. HAL-FC is useful at primary cystoscopy and resection of bladder tumors, during restaging in patients not previously evaluated with Cysview, patients with positive urine cytology and negative white light cystoscopy, and for surveillance cystoscopy after treatment of CIS.6 In practice the majority of our Cysview use has been incorporated in our treatment of CIS, typically in patients with positive cytology after treatment with BCG. Recently, we have incorporated this into our initial biopsy and resection of patients with newly diagnosed bladder cancer. This is not for repetitive use and is not a replacement for random bladder biopsies or other techniques used in the detection of bladder cancer.
Cysview reconstitution and patient preparationTop
Cysview is packaged in a kit containing 100 mg hexaminolevulinate HCL powder in a 10 mL glass vial, 50 mL of diluent (phosphate buffered saline), and a luer lock catheter adaptor, Figure 2c. Reconstitution is accomplished by aspirating the Cysview diluent using a 60 mL syringe with an 18 G blunt tipped needle. Ten milliliters of diluent is then injected into the glass vial containing Cysview powder. Without withdrawing the needle, the vial and syringe are gently rocked until all powder is visibly dissolved. The dissolved solution is then withdrawn into the 60 mL syringe containing the other 40 mL of diluent. Cysview is immediately ready for intravesical use, however if patient is not ready for treatment it may be stored for 2 hours at 2˚-8˚C. Prior to reconstitution, the Cysview kit may be stored at 20˚-25˚C.5
Reconstitution at our hospital is performed by the pharmacy after the patient has been admitted and assessed by our preoperative nurses. Once prepared, the Cysview is delivered by pharmacy and the patient is straight catheterized with a 16 Fr catheter using sterile technique and their bladder emptied of urine. All 50 mL of Cysview is slowly injected into the catheter and left to dwell in the bladder for between 1 and 3 hours. If left for longer than this time normal bladder mucosa begins to respond to the Cysview solution and lesions become difficult to distinguish, causing excessive false positive results and lowering the specificity. Cysview is not approved for use with silver-coated catheters.
After the Cysview has dwelled for approximately 1 hour the patient is taken to the operating room and prepared for rigid cystoscopy in the standard fashion. The utility of this technique is to direct biopsy and therefore these procedures are conducted in the operating room under adequate anesthesia. Rigid cystoscopy using the PDD system is performed using white light in a systematic manner identifying bladder anatomy and possible lesions requiring resection or biopsy. The blue button is then pressed for 1 sec and blue light cystoscopy is initiated. Before examining the bladder the scope is positioned at the bladder neck where a reddish/pink fluorescence is identified from a tangential effect confirming that Cysview has been applied properly. Systematic cystoscopy using blue light is then performed with 30 and 70 degree telescopes. When using blue light we have found that tangential artifact from the bladder wall can be minimized by directing the scope close and perpendicular to the bladder wall. Doing so makes lesions easily identifiable due to their bright red fluorescence. When lesions are identified we prefer to biopsy using white light as we feel the darker blue light illumination impedes depth perception. After initial fulguration of lesions, inspection using blue light should follow to identify any inadequately treated tumor left at the periphery. Fulguration under blue light has been safe in our hands, however resection should always be performed using white light due to decreased perception of depth and a perceivable strobe effect seen with quick movements. After resection blue light should be used to determine completeness of resection as a rim of fluorescence is often visible possibly identifying residual malignant urothelium.
Visibility within the bladder using blue light can be improved with basic troubleshooting already routine to the urologist during endoscopic procedures. Clear optics rely on proper cleaning and handling of equipment, adjusting camera focus and ensuring all devices are connected appropriately. Blood in the bladder significantly obscures vision to a greater degree than white light cystoscopy. Urine fluoresces green under blue light and therefore should be routinely drained from the bladder to improve visualization. Using a non-PDD telescope will result in a dark blue image. Poor patient selection can also result in poor visualization of bladder tumors using blue light as patients with inflammation from UTI, recent BCG therapy, or recent resection show diffuse pink fluorescence that limits the utility of HAL-FC and increases the incidence of false positive results.
After the procedure postoperative care is routine. Patients with visible tumor receive intravesical mitomycin therapy followed by void trial or discharge with a foley catheter depending on patient history. We have not experienced any recognizable adverse reactions from using Cysview, however local symptoms such as bladder spasm, dysuria, and hematuria were reported in clinical trials and were not significantly different than controls. The compound has been used extensively in thousands of patients in Europe for several years and is generally considered to be very safe. One case of anaphylactic shock has been reported in the literature that was possibly due to the compound.3
The treatment of superficial bladder cancer is often associated with a high rate of recurrence. “Blue light” cystoscopy offers a new tool in the management and treatment of NMIBC that may increase the detection of lesions not well seen under white light examination. We have incorporated it into our practice and have experience in almost 100 patients including those on clinical trials and in over 40 patients in routine care. Special points to consider during blue light cystoscopy are summarized in Table 1. A limitation is the fact that benign lesions such as cystitis cystica and other inflammatory lesions may fluoresce using this technique. In our experience the ability to increase the detection of sites of intravesical CIS is one of the most appealing aspects of blue light cystoscopy.
Our initial experience with this technology was as participants in a phase III, multicenter clinical trial. During this study 196 patients with either bladder lesions, positive urine cytology, or recurrent bladder tumor after treatment received white light cystoscopy with mapping of all detectable lesions followed by HAL-FC. Flat lesions were biopsied and fulgurated and papillary tumors were resected. Notably, of the 113 CIS lesions identified, 104 were seen with blue light and only 77 with white light. HAL-FC was determined to give additional information by the surgeon in 55% of cases and caused a change in planned treatment in 14% of patients.7 Other investigators have shown as many as 32% of their patients diagnosed with CIS by HAL-FC were missed by traditional cystoscopy with white light.8
Improved detection of superficial bladder tumors has proven beneficial by allowing for a more complete initial resection. Hermann et al recently performed a study where patients with suspected Ta or T1 bladder cancer were randomized to a control group receiving traditional TURBT with white light cystoscopy and an experimental group which received TURBT with white light followed by HAL-FC. Forty-five percent of patients with Ta and 43% of patients with T1 had residual tumor found by HAL-FC and the experimental group had a 35.5% relative reduction in tumor recurrence after 12 months.9 This is comparable to recent data published on 5 year and 8 year follow up showing that HAL-FC has a roughly 30% higher tumor recurrent free survival rate.3 The reduction in recurrence has lead to the European Association of Urology giving a grade B recommendation for fluorescence cystoscopy in patients who are thought to harbor high grade bladder tumors.10
HAL-FC using Cysview can improve detection of bladder tumors and long term experience in Europe with this technique has demonstrated its potential to decrease recurrence of bladder tumors. Now that “blue light” cystoscopy system is approved for use in the United States it adds a useful tool in the management of non-muscle invasive bladder cancer.
The authors report no conflict of interest associated with the publication of this paper.
Accepted for publication March 2012 Address correspondence to Dr. Leonard G. Gomella, Department of Urology, Thomas Jefferson University, 1025 Walnut Street, Suite 1112, Philadelphia, PA 19107


 Humber River Health
Humber River Health