
 Indexed in Index Medicus and Medline
Indexed in Index Medicus and MedlineLaser therapy has become an increasingly popular choice for resolving the lower urinary tract symptoms of benign prostatic hyperplasia (BPH). Introduced during the early 1990s,1,2 it results in a virtually bloodless operating field, permitting excellent visualization compared with transurethral resection of the prostate (TURP)3 and, thus, permitting a lower rate of complications and shorter hospital stay.4 The transurethral techniques and surgical landmarks used during laser surgery are similar to those used during TURP,4 which suggests a short learning curve for most practicing urologists. A recent innovation in photovaporization of the prostate (PVP) technology is the Evolve laser system (biolitec, Inc., East Longmeadow, Mass).2,5 It results in excellent tissue ablation and hemostasis,1-3,5,6 and complication rates have been low.6 In numerous PVP studies which this device was used show considerable improvement in maximum urine flow (Qmax)2,3,5,7 postvoid residual (PVR) urine,3,5,7 and urinary retention (UR) was seen,2 with minimal to no deterioration in erectile function.5,7 The Evolve laser system also allows for limited fluid absorption through venous sinuses,3 making it particularly suitable for patients with cardiac conditions, which often accompany BPH.8 Because it is effective under regional local anesthesia,9 the need for hospitalization is limited; excellent follow up results have been achieved in men hospitalized for as few as 57 to 24 hours.5 These characteristics suggest that the 980 nm/1470 nm laser system may be suitable for office settings.
BPH treatments performed at Urologic Associates of Montgomery County, a division of Academic Urology of PA, LLC in East Norriton, Pennsylvania, with an office based treatment protocol for the Evolve laser system and local anesthesia were reviewed. Additionally, cases were performed at The Stone Center of New Jersey LLC, Short Hills, New Jersey, an ambulatory care facility with anesthesiologist controlled IV sedation.
We reviewed medical records of 87 patients with BPH who underwent surgery in the offices of one urologist from Urologic Associates of Montgomery County in East Norriton Pennsylvania as well as 93 patients performed at The Stone Center of New Jersey. A broad range of comorbidities were included; the only exclusion criterion in New Jersey was an atonic neurogenic bladder. The non sedation setting in Pennsylvania also excluded patients with pacemakers and defibrillators. Preliminary findings suggest favorable improvement in symptoms and patient satisfaction in men.
Equipment
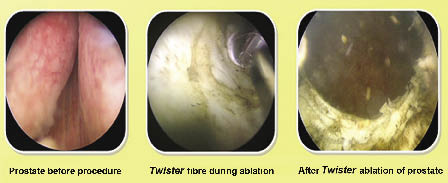
The Evolve Dual (980 nm/1470 nm) laser system, Figure 1, was set at 150W in continuous mode, with up to 200W of available energy, giving the physician the flexibility to increase or decrease the energy based on surgical needs. The energy can be changed at 1W or 5W increments any time the laser is not firing. We used a 24 Fr continuous flow cystoscope fitted with a 300 telescope and visual obturator for optimal visualization. We ensured that the cystoscope had a 7.5 Fr working channel for the Twister fiber (biolitec, East Longmeadow, MA, USA), Figure 2.
Preoperative patient preparation
All patients had an appropriate preoperative work up prior to consideration of the procedure.
Preoperative anesthesia
Patients were given Levaquin (levofloxacin) 500 mg to take 24 hours before the procedure. On the day of the procedure, they underwent a standard BPH work up, including a history and physical examination, and in some cases transrectal ultrasound of the prostate. Thirty to 60 minutes before the procedure, they were directed to empty their bladders and take an age appropriate dose of diazepam (> 75 y: 5 mg; ≤ 75 y: 10 mg) and oral Percocet (acetaminophen and oxycodone). Fifteen minutes before the procedure, 50 mL of cold 2% lidocaine was instilled into the drained bladder and the penis was clamped. We then administered 10 cc of 2% lidocaine gel intraurethrally and a combination of 1% lidocaine and 0.5% marcaine (30 mL each) transrectally to achieve prostatic and transurethral blockade.
In New Jersey, an office extension lease arrangement allowed for office based billing rates by the urologist. Anesthesiology billed separately for directing indicated sedation and pain management.
Preoperative anesthesia (Pennsylvania)
Patients were also given Levaquin (levofloxacin) 500 mg to take 24 hours before the procedure. On the day of the procedure, they too underwent a standard BPH work up, including updated history and physical examination. The surgeon here did not routinely perform transrectal ultrasound of the prostate in this setting. Ninety minutes before the procedure, the patients were instructed to take similar doses of both diazepam and oral Percocet.
This surgeon only administers 10 cc of 1% lidocaine gel intraurethrally to achieve adequate urethral analgesia. This surgeon achieves maximal analgesia by utilizing intraoperative iced saline throughout the entire procedure, along with a preoperative transurethral intraprostatic block with lidocaine (discussed in surgical procedure section).
Patient positioning
Each patient was prepped and draped for a standard cystoscopic procedure in the appropriate leg stirrups and fitted with safety glasses to prevent laser exposure.
Both surgeons began by inserting the outer sheath of the cystoscope into the urethra through the visual obturator followed by the laser bridge. After distending the bladder with iced saline solution, we moved the scope forward until its tip was in the bladder. At this point, an intraurethral prostatic block was performed through the cystoscope using a flexible needle to introduce 1% lidocaine into the gland was done in Pennsylvania. No further anesthetics were required in New Jersey.
Both surgeons then inserted the Twister laser fiber until it was near the tip of the scope and performed a preliminary cystoscopic examination. Beginning at the level of the bladder neck, we began vaporizing tissue from the surface of the median lobe, sweeping the fiber slowly and continuously in a gentle rotation movement in a 5 o’clock-to-7 o’clock direction, keeping the fiber in direct contact with prostatic tissue. When the median lobe was reduced, we proceeded to the right lateral lobe, using the same technique, and then to the left lateral lobe. A slow continuous motion assures hemostasis, constant reassessment prevents loss of position and possible trigonal or sphincteric injury. The anterior aspect of the prostate was always additionally vaporized by the surgeon in Pennsylvania.
Once it was felt that the procedure was complete, we retracted the cystoscope to the level of the verumontanum and looked toward the bladder neck to confirm the presence of a TURP-like cavity (sample cavity appears in Figure 2). The patient was then checked for hemostasis with irrigation off, fitted with a Foley catheter, and sent home with a 6 day supply of Levaquin (500 mg/d). Patients in Pennsylvania were only given an additional 2 days of Levaquin. Patients were to return the next day to have their catheters removed.
Through the use of the Evolve laser systems, we have also seen a dramatic change in PVR, Qmax, IPSS, and QoL. Similar changes were also seen in men with large prostates, although their laser exposure time was somewhat longer. Complications were limited primarily to vesicular neck contracture and UR, respectively. Less than 2% of patients required TURP to correct complications.
With the Evolve laser systems, only one fiber was needed to perform each case, with the exception of one case where an additional fiber was used to treat an extremely large prostate. The second fiber was issued at no charge due to “biolitec One Fiber Guarantee”.
Recovery nurses noted little to no bleeding postoperatively, this cut down on postop supplies to control bleeding, which is common with other laser or RF technologies.
The Evolve Dual (980 nm/1470 nm) laser system offers the benefits of a short learning curve, higher ablation rates, excellent hemostasis and portability. It also allows for excellent visualization of the surgical field, due to the bloodless nature of the procedure using the dual wavelengths. Additionally, we have observed and demonstrated that the Evolve Dual (980 nm/1470 nm) laser system has excellent efficacy and safety for use in either the office or ambulatory care facility, minimizing the need for inpatient procedures and hospitalization. These factors all point to an excellent surgical management of BPH, along with a tremendous reduction in the cost of care.
Dr. Brian D. Rosenthal is a consultant for biolitec, Inc. in East Longmeadow, MA, USA.
Dr. Joseph V. DiTrolio - None.
Accepted for publication March 2012
Address correspondence to Dr. Joseph V. DiTrolio, 556 Eagle Rock Avenue, Suite 204, Roseland, New Jersey 07068 USA


 Humber River Health
Humber River Health