©TheCanadian Journal ofUrology™: International Supplement, April 2014
suitablephosphonate (MDPmost commonly) – remain
themainstayofimagingmetastaticprostatecancer. Bone
scans are typically carried out to identify metastatic
disease. Bone is thesiteofmetastases in90%ofpatients
withmetastaticprostate cancer.
4
TheBoneScan Index,
an estimate of metastatic bone,
5
is a metric that has
shownpromiseasapharmacodynamicbiomarker
6
and
thesemeasurements have been automatedwith some
success,
7
though the overall technique remains rather
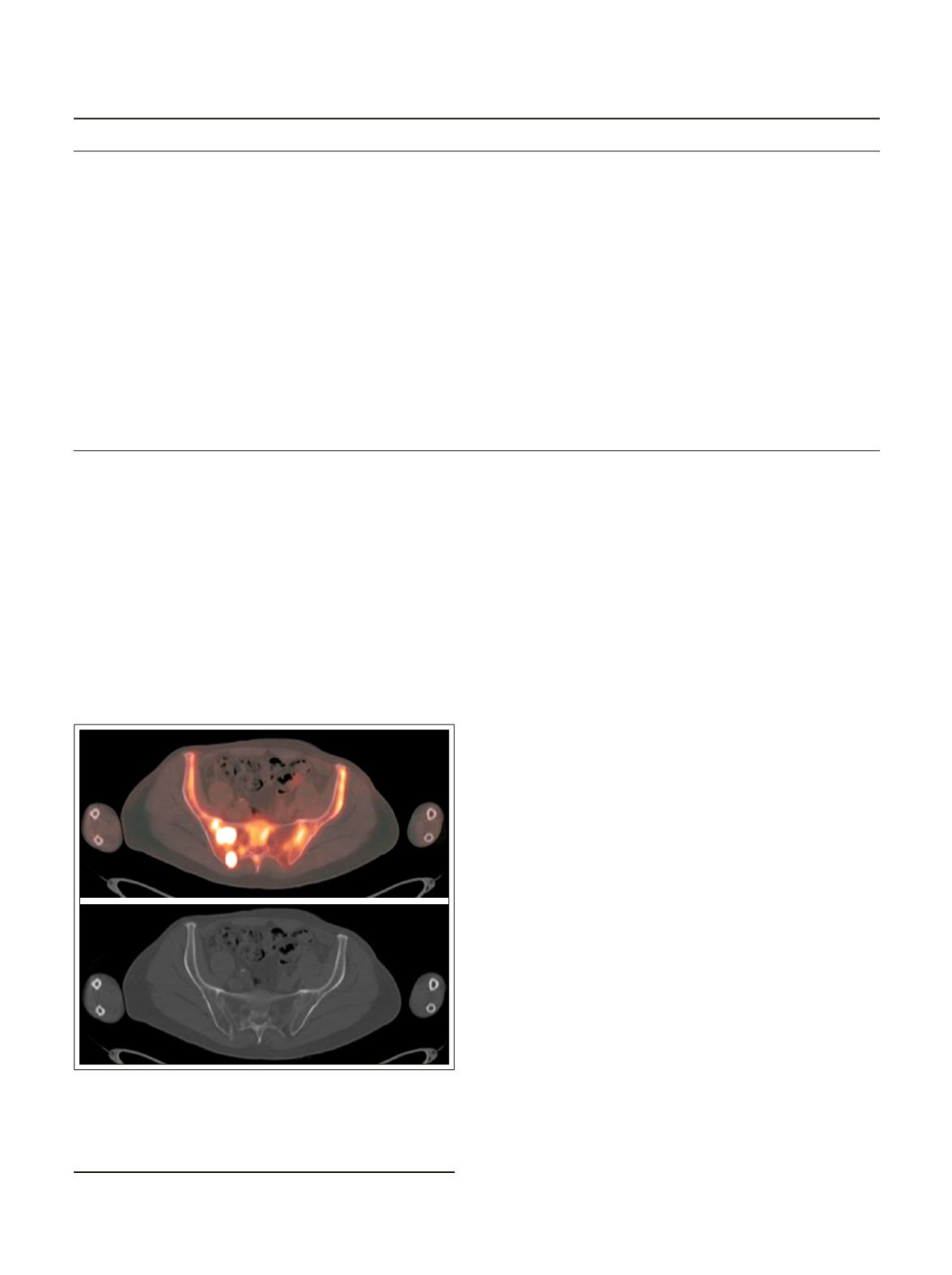
cumbersometouse. Sodiumfluoride-18([18F]NaF)PET,
Figure 1, is generally consideredmore sensitive than
bone scintigraphy, though comprehensive prospective
comparisonsarelackingandarenowbeingaddressedin
aNationalOncologicPETRegistry(NOPR)trial.
8
Several
small studies have demonstrated the greater accuracy
of NaF PET in the detection of bonemetastases.
9,10
In
particular,NaFhasahigherspecificitythanconventional
bonescintigraphy, leadingto itshigheraccuracy. Table1
illustrates the main differences between these two
imagingmodalities.
Computed tomography (CT) iscarriedout toassess
extra-osseous tumor involvement, thoughbone lesions
mayalsobe identifiedasblasticormixed lesions. Soft
tissuediseaseisusuallynodal, identifiedusingCTscans,
anddoesnot contributemuch todiseasemorbidity.
11
Identification of disease outside the prostate bed
by one or more of the imagingmodalities described
above leads to systemic therapy. Such therapy is
followed with serial bone scans, though these are
useful primarily to identify progression of disease.
The frequency with which bone scans are carried
out is highly variable, based on reimbursement as
well as on patient characteristics – elderly patients
with underlying bone and joint disease may have
confounding results, limiting the utility of the bone
scans; usually, bone scans are carried out onlywhen
PSA changes are such that treating physicians need
objective evidenceof osseousmetastases.
Imagingofcastrationresistantprostatecancer
Metabolic imaging
The mainstay of imaging prostate cancer remains
the bone scan, either using scintigraphy or PET/CT.
However, severalmolecularagentsarebeingstudied,
particularlywithPET/CT.
TABLE 1.
Maindifferencesbetween two imagingmodalities
Bone scanwith
BonePET scanwith
Tc-99mphosphonate
F-18 sodiumfluoride (NaF)
Radionuclide
Tc-99m
Fluorine-18
Half-life
6hours
2hours
Radiationdose
5milli Sievert
2.5milli Sievert
Time for scan
Typically 30minutes,
Typically 15minutes, starting 30minutes
starting 2-3hours
after injection
after injection
Cost
Approved imaging study
Carriedout underNOPR, forMedicarepatients;
costs variable, typicallymore expensive than single
photonbone scan
Accuracy
High
More sensitive and specific
Figure 1.
Bone PETwith fluorine-18 (F-18) sodium
fluoride in apatientwithCRPC. The lesions seenon
the PET/CT are not always evident on theCT alone.
A.
FusedPET/CT.
B.
CTbonewindow.
A
B
43
LeungETAL.


