©TheCanadian Journal ofUrology™: International Supplement, April 2014
Bander et al developed an antibody, J591, that
targets the extracellular domain, and this antibody,
whiledeveloped initiallyas a therapeutic, has shown
promise as an imaging agent.
31
PSMA has several
advantages as a target, since its over-expression is
directly proportional to the de-differentiation of the
prostatecell – it is thusexpressed ingreaterquantities
on thecastrationresistant than in the -sensitivecancer
cell.
32
While initial imaging studieswere carried out
with indium-111,with the inherent limitationsofsingle
photon scintigraphy, recent reports have suggested
thataccuracyofdetectionmay improvewithPETusing
zirconium-89 labeled anti-PSMAantibody.
33
Small molecules that target PSMA are also being
evaluated. They have shown utility in detection,
and an advantage compared to the macromolecular
antibody is that clearance is rapid and thus imaging
can be carried out the same day with more widely
availablepositron emitters.
34,35
Magnetic resonance imaging (MRI)
The lackofwidespreadutilizationofwholebodyMRI
has limited the number of studies that have evaluated
the role of this imagingmodality in CRPC, Figure 3.
Morefrequenthasbeenassessmentofindividuallesions,
usingfunctionalparametersobtainedbyadvancedMRI
techniquesincludingdynamiccontrastenhancedorDCE
MRI, and diffusion-weighted or DW-MRI. Bothmay
havea roleaspharmacodynamicbiomarkers.
Bonemetastaseshavebeenevaluatedusingboththese
methods.
36
DCEMRIhasbeenusedto identifymarrow
infiltration by prostate cancer; the abnormal marrow
has higher values of a semi-quantitative parameter
thatmeasuresflow.
37
Diffusionweighted imaginghas
beenused both to characterizemetastases
38-40
and as a
predictive
41
andpharmacodynamic
42,43
biomarker.
Hyperpolarizednuclei haveproperties that permit
MRIwith extremelyhigh sensitivity, and carbon-13 is
a hyperpolarized nucleus that has been successfully
studiedinhumanslabeledtopyruvate. Hyperpolarized
C-13 labeledpyruvatehas shownpromising results in
imagingprostatecancer,
44
andstudiesareunderway to
address itsutility.
Timing
Whenshouldimagingbecarriedout?Theonlyconsensus
documentforCRPCinthisregardisunclear.
45
Bonescans
should be repeated preferably only after the end of a
courseof therapy. Abone scan that showsprogression
mayrepresentaflareresponse,andthusunlessthereare
multiplenew lesions (usually twoormore) that persist
in a followup scan obtained at least 6weeks later, the
scancannotbeconsideredtobeprogression. Bonescans
moreover rarely demonstrate a reduction in uptake
intensityor lesionnumber followingsuccessful therapy,
andhencecannotbeusedtoreliablydocumentresponse.
Metabolic and receptor imaging, particularly
with PET andMRI, may have an important role in
assessment of therapy response. These techniques
havebeenshown tobeextremelypromising,but there
are few studies that have systematically evaluated
thesenovelmethods, and the cost constraintsofmost
modern imagingtechniquesprecludetheirwidespread
utilization especially given the low cost of currently
availablebiomarkersforestimationofextentofdisease.
Biochemical change is however not rapid. The
ultimate value of the novel imaging biomarkersmay
therefore be not in their utility as pharmacodynamic
biomarkers,butaspredictiveorprognosticofaggressive
disease, or indeed as EARLY pharmacodynamic
biomarkers. This last may be particularly useful as
costlyandunnecessarytherapymaywellbeavoidedby
anearly indicationof thefutilityofaparticular therapy.
Conclusion
Imaging castration resistant prostate cancer is still in
its infancy. Inparticular, bonemetastases remainnon-
measurable, evaluatedbybone scans that are sensitive
but not specific. Novel imaging techniques that assess
extent of disease in the whole body are limited to
molecularimaging,particularlyPET/CT. MRIcancarry
outassessmentofindividuallesions,withpredictiveand
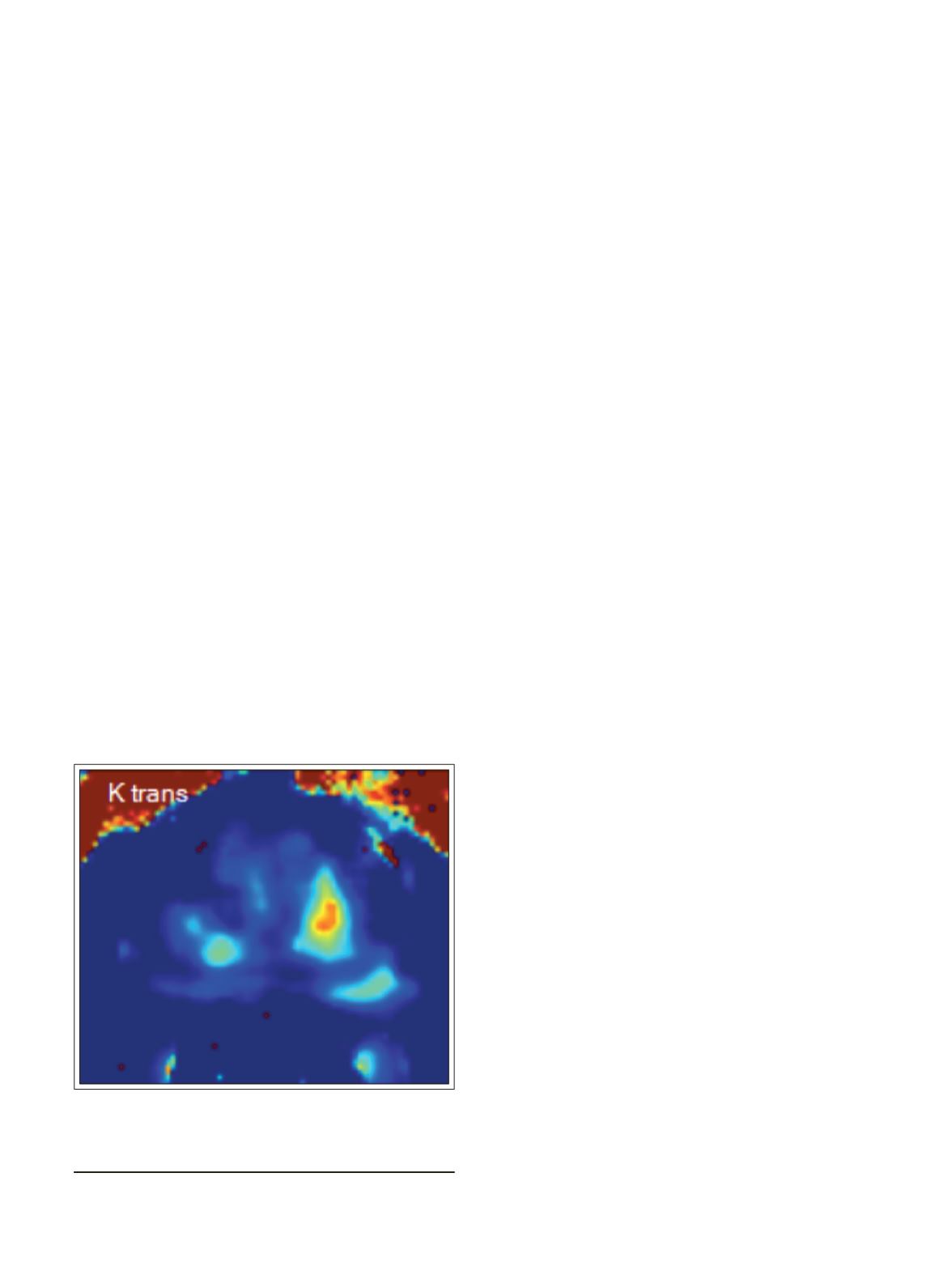
Figure 3.
Parametric image of K
trans
, a measure of
vascularity inaprostate. Theredarearepresentsahigh
Gleasonprostate cancer.
45
LeungETAL.


