©TheCanadian Journal ofUrology™: International Supplement, April 2014
patients were underrepresented in the SEUG 9901
20
trialwhichconcludednon-inferiorityofIADTtoCADT
in this prostate cancer state. Similarly, for patients
with biochemical relapse after radiotherapy, there is
no evidence that early ADT in lower risk relapsing
patients is beneficial—and higher risk patients were
aminoritypopulationof thePR7 trial,
21
which found
non-inferiority of IADT to CADT in this prostate
cancer state. In patients with metastatic disease,
CADT remains the standard of care as SWOG 9346
22
wasstatistically inconclusive,findingneither thenon-
inferiority of IADT to CADT nor the superiority of
CADT toIADT. Althoughmeta-analysesofIADThave
beenpublished,
12,13
this approachhas limited clinical
relevanceas itcombinesresults fromseparateprostate
cancer disease states and contaminates the results of
veryhigh-quality trialswith low-quality trials.
Castration related symptoms including ED,
low libido, hot flushes, fatigue, and headaches are
improvedby IADTduringoff-treatmentperiods. This
likely relates to improvements in testosteroneduring
off-treatmentperiodsalthoughaplaceboeffectremains
apossible contributor.
If symptom management is unsuccessful,
considerationshouldbegivenas towhetherwatchful
waitinganddeferredADT isanappropriateoption for
thesepatients at this stateof hisdisease—namely the
patientreceivingprimaryADTorADT forbiochemical
relapse following local therapy. If some formofADT
isstill felt tobenecessary, IADThasan indicationhere
asacompromisebetweenuncertainsurvivaloutcomes
inhigherriskpatientsand improvedsymptomatology.
Although there are small variations inhow IADT is
appliedamongstphaseIIItrials,thegeneralprinciplesare
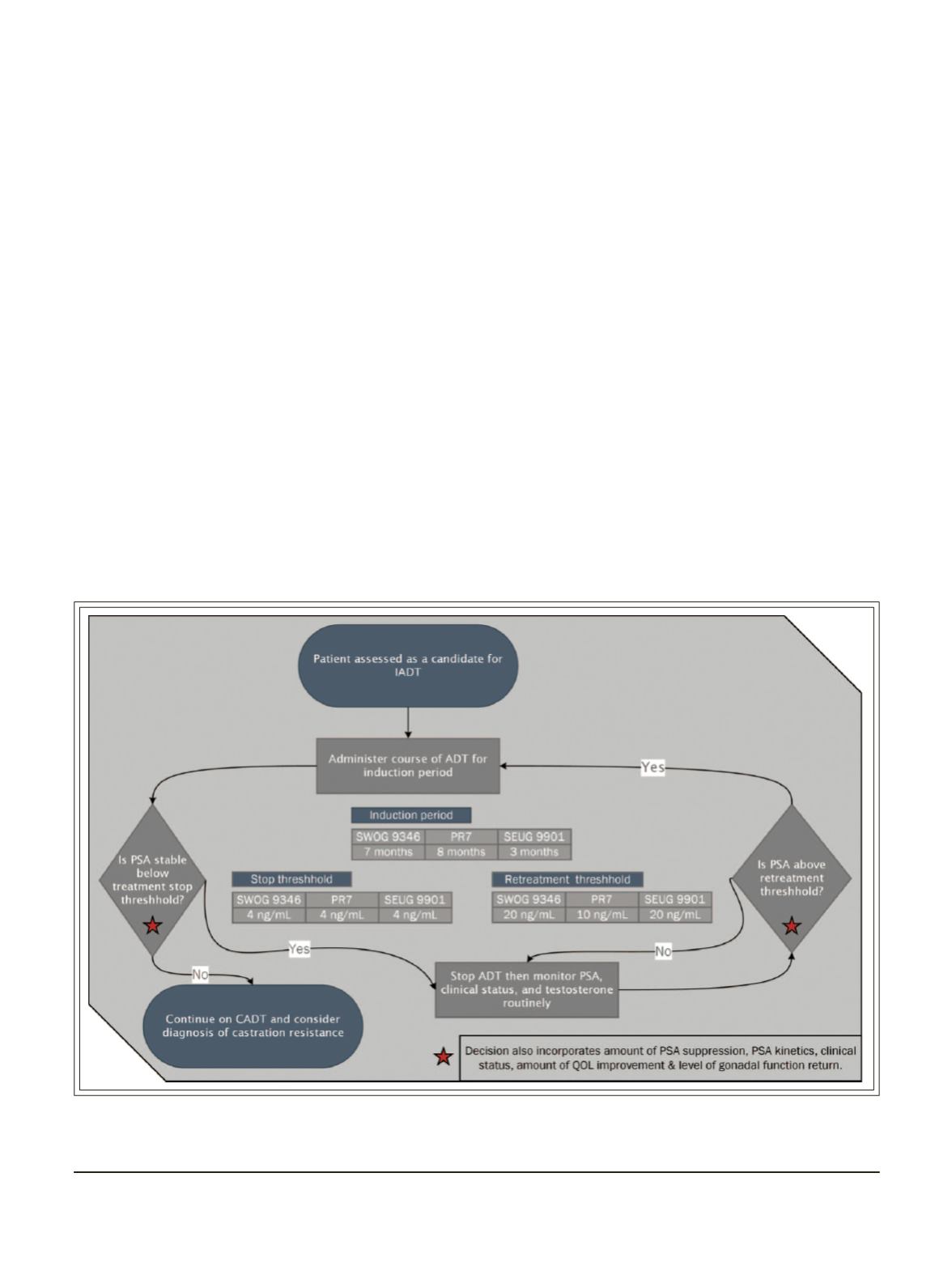
thesame,Figure2.AsillustratedinFigure2,IADTbegins
with an inductionperiod ofADT administration. This
periodmaybeasshortas3months(asseenintheSEUG9901
trial,oraslongas8monthsasinthePR7trial). If,afterthe
inductionperiod,PSAissuppressedadequately(4ng/mL
in SWOG 9346, PR7, and SEUG 9901) then ADT
administrationmaybe halted. Prostate specific antigen
levelsandclinical statusareclosely followed,withADT
resumed on certain triggers such as symptoms or a
PSA rise to 10-20ng/mL (10ng/mL inPR7, 20ng/mL
or baseline in SWOG 9346 and 20 ng/mL in SEUG
9901). If PSA is again suppressed to 4 ng/mL or less
Figure 2.
Clinical protocol for intermittent androgendeprivation therapy administration.
ADT= androgendeprivation therapy; IADT= intermittentADT; CADT= continuousADT; PSA=prostate-specific antigen.
SWOG 9346, PR7 andSEUG 9901 are the three largest phase III trials comparison IADT andCADT.
34
Intermittent androgen deprivation therapy for prostate cancer: translating randomized controlled trials into
clinical practice


