©TheCanadian Journal ofUrology™: International Supplement, April 2014
testosterone to castrate levels for the duration
of therapy. Alternatively, intermittent androgen
deprivation therapy (IADT) involves cycles of ADT
that are interruptedby injection-free intervalsduring
which time testosterone levels are permitted to rise
abovecastrate levels. Testosteronerisesslowlyduring
theseperiodsandmanypatientswillhave incomplete
recoveryof their pre-ADT testosterone level.
The first description of IADT in clinical practice
was reported by Klotz et al,
4
who reported on
20 patients with symptomatic metastatic disease
treated intermittently with diethylstilbestrol (DES).
Independently, Bruchovsky et al,
5
through their
workwith theShionogimousemammary carcinoma,
hypothesized that intermittent therapycouldprolong
time to castration resistance because CADT may
preferentially enrich castration resistant stem cells.
Theoriessurrounding thebeneficialeffectsof IADT
prompted a number of recent phase III trials.
6
The
primary hypothesis of IADT is that the testosterone
reboundduring treatment-free intervalsof IADTmay
ameliorate some the adverse effects of ADT. These
includecastrationrelatedsymptomsand theirnegative
impact on health-related quality-of-life (HRQOL). It
has also been hypothesized that IADT potentially
reduces some of the bone and cardiovascular health
sequelae of ADT. Finally, it has been proposed that
cyclic testosterone fluctuations during IADT do not
enrich cells with a castration resistant phenotype,
potentially improving oncologic outcomes.
5
This
review seeks to critically analyze how the available
phase III trial evidence supports or refutes these
theories at variousprostate cancerdisease states.
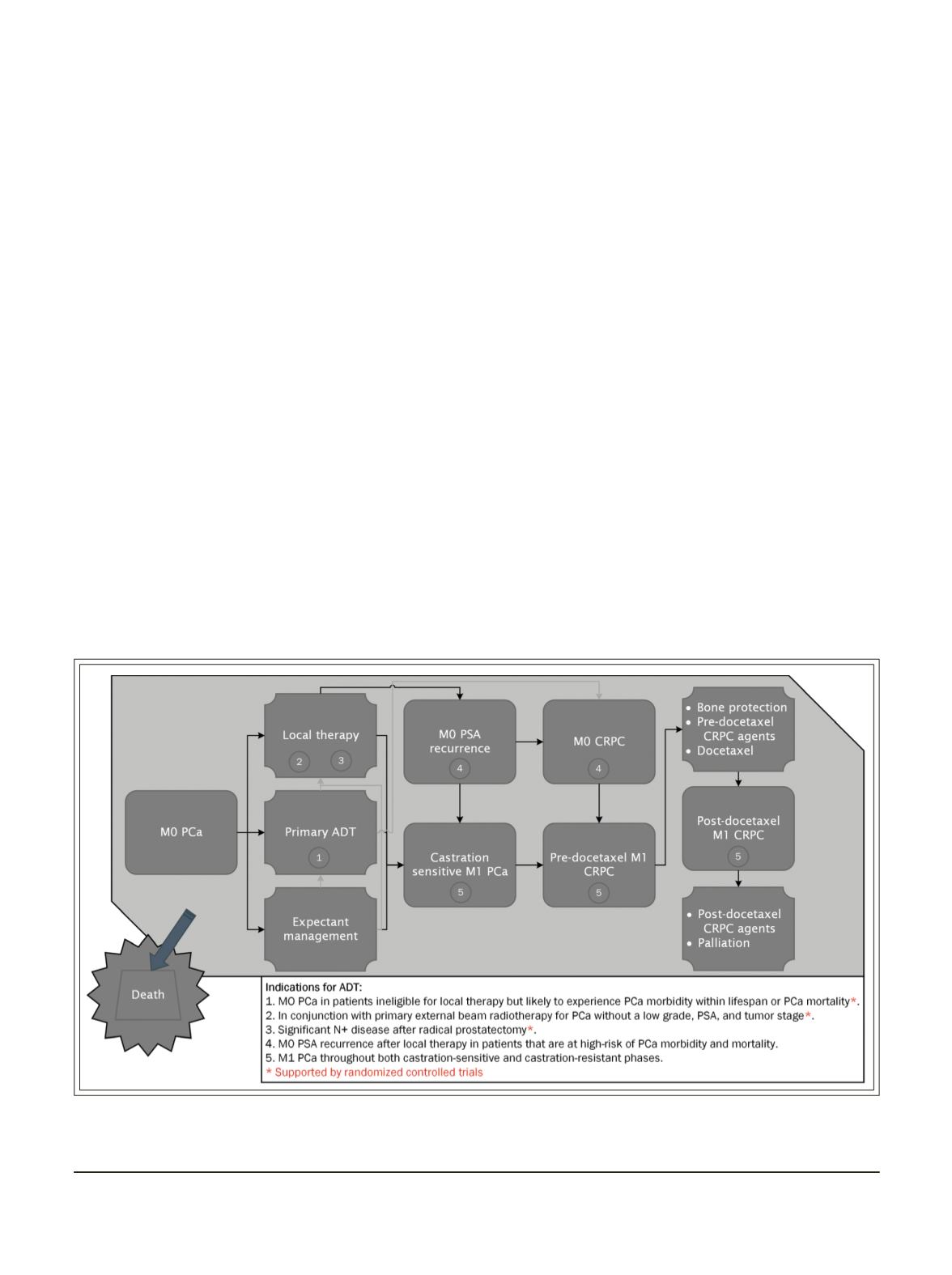
Adisease statemodel of prostate cancer
Scher andHeller
7
proposed that prostate cancermay
bemodeledasaseriesofdiseasestates throughwhich
patientsmayprogress, ranging from localizedprostate
cancer to castration resistant prostate cancer (CRPC)
that progresses after chemotherapy, Figure 1. Death
mayoccurduringanydiseasestate,and therefore,does
not necessarily result directly from prostate cancer
due to its prolonged natural history and competing
causesof death. Thegoalsof prostate cancer therapy
during anydisease state includeprolonging survival
andoptimizingHRQOL.
Prostatecancerundergoesareduction inglandsize
and an increase in interglandular connective tissue
during ADT.
8,9
Although residual tumor remains
9
and an inevitable progression to CRPC occurs,
tumor-related symptom reduction is experienced on
Figure 1.
Indications for androgendeprivation therapy at different states of prostate cancer.
11
PCa=prostatecancer;CRPC=castrationresistantprostatecancer;ADT=androgendeprivation therapy;N+=nodalmetastases;
PSA=prostate-specific antigen;M0=non-metastatic;M1=metastatic
29
DasonETAL.


