©TheCanadian Journal ofUrology™: International Supplement, April 2014
Figure 1. Thismode of therapy avoids any need for
concomitant antiandrogen flare protection although
some clinicians prefer to continue to use oral
antiandrogensevenwithdegarelix forchronicadrenal
androgenblockade.
Abarelix
Abarelixwas thefirst-in-classLHRHpureantagonist
that was Food and Drug Administration (FDA)
approved inDecember2003 to treatadvancedprostate
cancer.
3
While very effective at inducing a very
rapid lowering of serum T, it was found to cause a
hypersensitivity reaction in a very small percentage
of patients and received a “BlackBoxWarning” from
theFDAin late2004. Shortly thereafter inearly2005, it
wasdiscontinued from theUnitedStates (U.S.)market.
The remainder of this chapter will refer to degarelix
since it is the only agent in the class that is currently
FDA-approved and commercially available.
FDAapproval of degarelix
Asecond-in-classpureLHRHantagonist,degarelix,was
FDA-approved inDecemberof2008.
5
Nowwithover5
years of clinical use, degarelixhasnot beenassociated
withanyseriousadverseeventsandhassteadilygained
somemarket share as a parenteral ADT agent. More
recent followupof thedegarelixpivotal phase III trial
inwhichtheagentwascomparedtomonthly leuprolide
suggests that itmaybemore effective than leuprolide
forpatientswithmetastaticdiseaseat studyentry.
7-9
Degarelix (Ac-D-2Nal-D-4Cpa-D-3Pal-Ser-4Aph(L-
hydrorootyl)-D-4Aph(carbamoyl)-Leu-Ilys-Pro-D-Ala-
NH
2
) isasynthetic, lineardecapeptideamideanalogue
of endogenous GnRH. This compound is produced
by insertion of seven exogenous amino acids, five of
whichareD-isomeraminoacids. Degarelixbindstothe
pituitaryGnRHreceptors, therebyreducing therelease
of gonadotropins and consequently testosterone, and
importantly this binding is reversible.
The initial dose-finding studies with degarelix
suggested that 240 mg appeared to be the optimal
starter dose, as this regimen resulted in castrate
testosterone levels in> 96%of patientswithin 3days.
This led to a 1 year, multicenter, randomized, open-
label, parallel-group, phase III trial (CS21)designed to
demonstrate the statistical non-inferiorityof degarelix
versus the LHRH receptor agonist leuprolide.
5
This trial enrolled 610 patients with all stages of
histologically confirmed prostate cancer and eligible
forADT. The study randomized patients to a starter
dose of 240 mg sc degarelix followed by monthly
maintenance doses of either 80 mg (240/80 group,
n = 207) or 160 mg (240/160 group, n = 202) or to
monthly leuprolidedepot 7.5mg im (n=201). For the
patients intheLHRHreceptoragonistgroup,CABwith
an antiandrogen could be added at the investigators’
discretion.
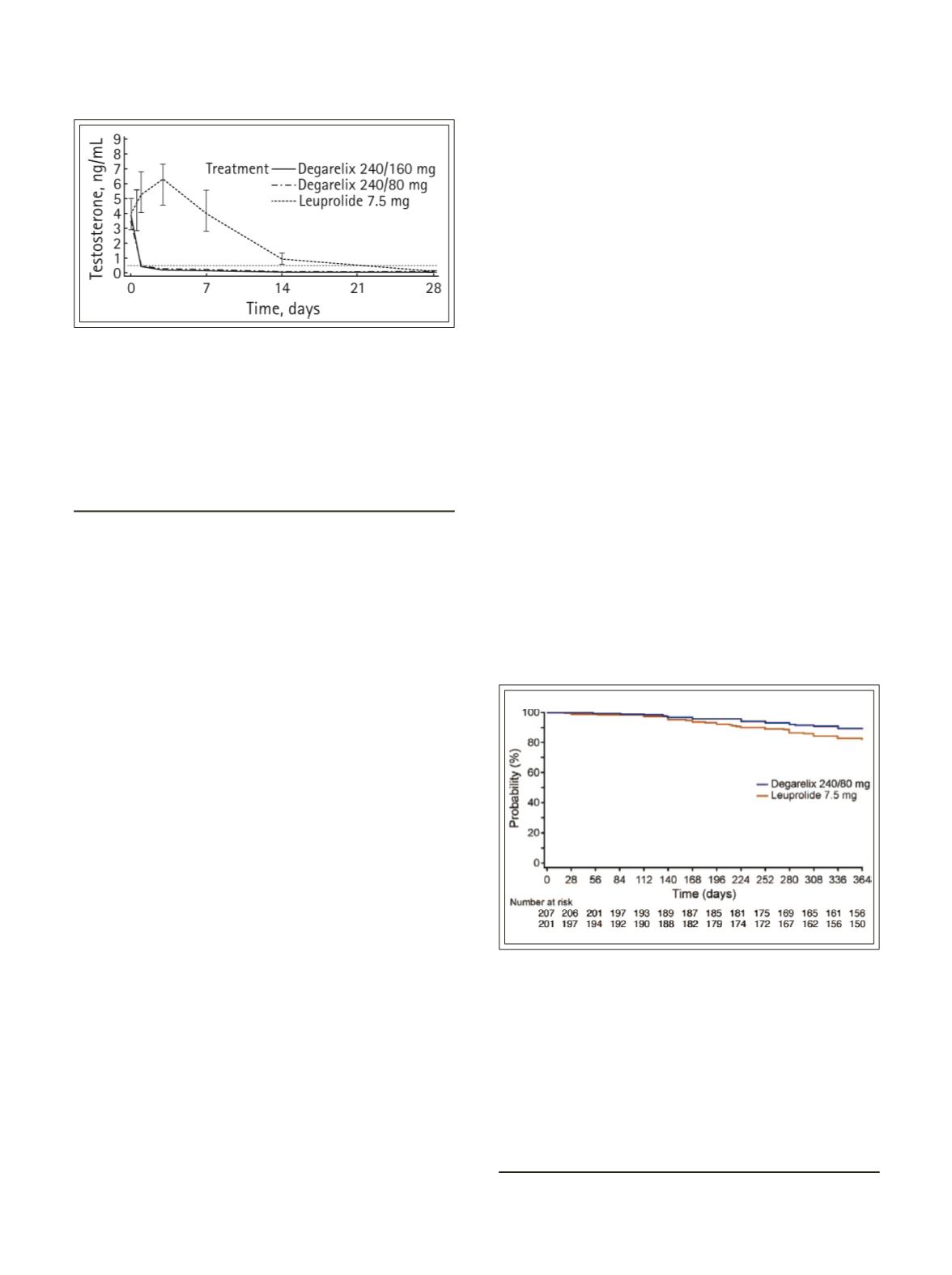
Figure 1.
Comparison of serum testosterone levels
duringfirst28daysofdegarelixversus leuprolide in the
KlotzetalpivotalphaseIIIclinicaltrialwhichformedthe
basisforFDAapprovalofdegarelix. Notethetestosterone
surgeintheleuprolidepatients(dottedline)comparedto
therapidtestosteronesuppressioninthedegarelixtreated
patients. Thisisthekeyclinicaldatasupportingdegarelix
use inclinicalpractice.
5
Reprintedwithpermission.
Figure2.
In followupof theKlotzet al phase IIIRCT
comparing degarelix versus monthly leuprolide, the
disease-free survival in the patients with metastatic
disease was statistically improved for degarelix-
treated men compared to leuprolide-treated man at
1 year follow up. This data is in the peer reviewed
literature (Tombal et al)however, thefindings remain
controversial. It is intriguingbutmust be considered
hypothesisgeneratingand isnotconsideredvalid level
I evidence.
8
Reprintedwithpermission.
23
Moul


