© The Canadian Journal of Urology™; 21(Supplement 2); June 2014
Figure 2.
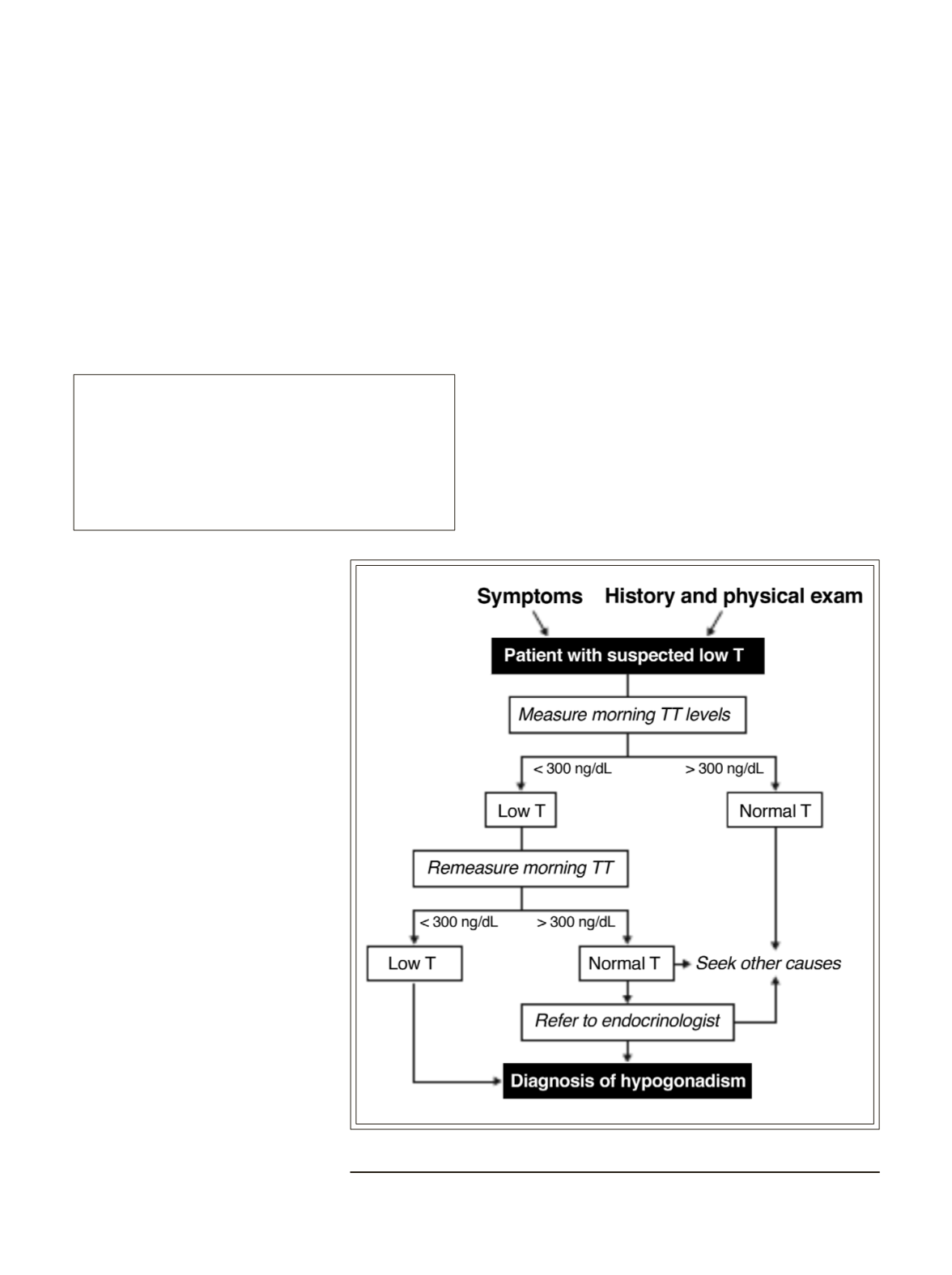
Evaluation of testosterone deficiency.
11,12,32,40,42,47
National and international guidelines concur in
recommending TD screening for men deemed at risk
due to coexisting illnesses, Table 2. The conditions
include infertility, type 2 diabetes, metabolic syndrome,
chronic obstructive pulmonary disease, inflammatory
arthritis, cardiovascular disease, and chronic use of
glucocorticoids and opioids.
11,13,14,42
Clinicians should
maintain a high index of suspicion of TD in patients
with these comorbidities. Even those at-risk patients
who report no symptoms typical of hypogonadism
require a thorough clinical and biochemical workup
for TD.
*Key learning point:
For menwith sellar mass, HIV-associatedweight
loss, low trauma fracture, or use of medications
that affect testosterone production, measurement
of testosterone should be considered regardless
of hypogonadal symptoms.
high-yield questions to ask in the TD work up.
Even so, the current array of questionnaires are too
time-consuming for most primary care clinicians to
routinely utilize, especially given the lineup of other
screeners suggested for primary care (for depression,
dementia, and cancer, to name a few) that compete
for time and resources. Newer screeners for TD are in
development with fewer questions, and thus shorter
completion time; these are likely to become available
in the next 2 years.
This algorithm, Figure 2, may initially appear to be
a bit simplified. Yet it is useful for the primary care
clinician with perhaps the addition of two caveats.
First, if total testosterone is low on the first draw and
in a patient with at least a single symptom of TD
(T < 300 ng/dL) then a secondmorning (7 am to 11 am)
draw must be done with a LH added to distinguish
primaryfromsecondaryTD. IftheinitialTis<150ng/dL,
then one should add a prolactin level to this second
test. Second, if the prolactin returns at > 35 ng/mL,
one should order an MRI of the pituitary to determine
There is little support for the
use of formal questionnaires
as a screening method for TD,
especially as an isolated method
in the work up. TheAgingMales’
Symptoms and the Androgen
Deficiency in Aging Men scales,
two of the better known symptom
inventories used in TD screening,
demonstrate high sensitivity for
identifying men with TD but
very low specificity (< 40%),
45,46
making them unreliable for
screening. In a recent trial with
587 community-dwelling men
aged 60-80 years with known
TD, the scores from these scales
correlated more closely with
age than with testosterone, and
they did not reflect changes
in symptoms after a 6 month
regimen of testosterone therapy.
45
This latter finding is unfortunate
because some clinicians find
the instruments useful as a
reference for evaluating the
effects of treatments.
42
However,
the screeners may be helpful
in identifying patients with a
high likelihood of TD, and for
educating the clinician about
45
Testosterone deficiency: myth, facts, and controversy


