© The Canadian Journal of Urology™; 21(Supplement 2); June 2014
TD prevalence in men with comorbidities, most
significantly in those who were obese or had diabetes,
hypertension, rheumatoid arthritis, hyperlipidemia,
or osteoporosis. The odds of having low testosterone
levels were 2.4 times higher for obese men, 2.1 times
higher for men with diabetes, 1.8 times higher for men
with hypertension, and 1.5 times higher for those with
hyperlipidemia.
15
As epidemiologic research continues inmiddle-aged
andoldermen, thewide disparities inprevalence figures
should begin to narrow. Meanwhile, more specific
findings regarding TD in younger men are appearing.
Obesityanddiabetesare themost commoncomorbidities
but others, such as hypertension, dyslipidemia, and
chronic opiate use, steroid abuse, stress, and possibly
genetic factors also drive testosterone levels.
20,21
As
discussed below, long termopiate use and chronic pain
are comorbidities of TD seenwith increasing frequency
in primary care settings.
Most importantly, thebiologicpotential of testosterone
therapy to interfere with spermatogenesis, a particular
concern in younger men being treated for TD must be
noted in the primary care setting. Use of a low dose of
human chorionic gonadotropin (hCG) in conjunction
with testosterone replacement is a potential means of
protecting spermatogenic function while improving
testosterone levels.
22
Comorbidities
The links between TD and more serious medical
conditions are only beginning to be explored. At the
very least it can be said that comorbid illnesses seem
to explain some of the decline in testosterone that is
attributed to aging. At most, one can identify specific
conditions that have strong epidemiologic associations
with TD, Table 2. Arecent analysis of HIM data based
on free testosterone levels revealed that 40% of obese
men and 50% of obese men with type 2 diabetes
(45 years and older) were testosterone-deficient.
23
Connections between cardiovascular disease and
TD are suggested by TD’s associations with diabetes
and metabolic syndrome, and by such findings as an
inverse relationship between testosterone level and
aortic atherosclerosis, which was seen among middle-
aged and older men in the RotterdamStudy.
24
Low free
testosterone has also been associated with abdominal
aortic aneurysm in community-dwelling men aged
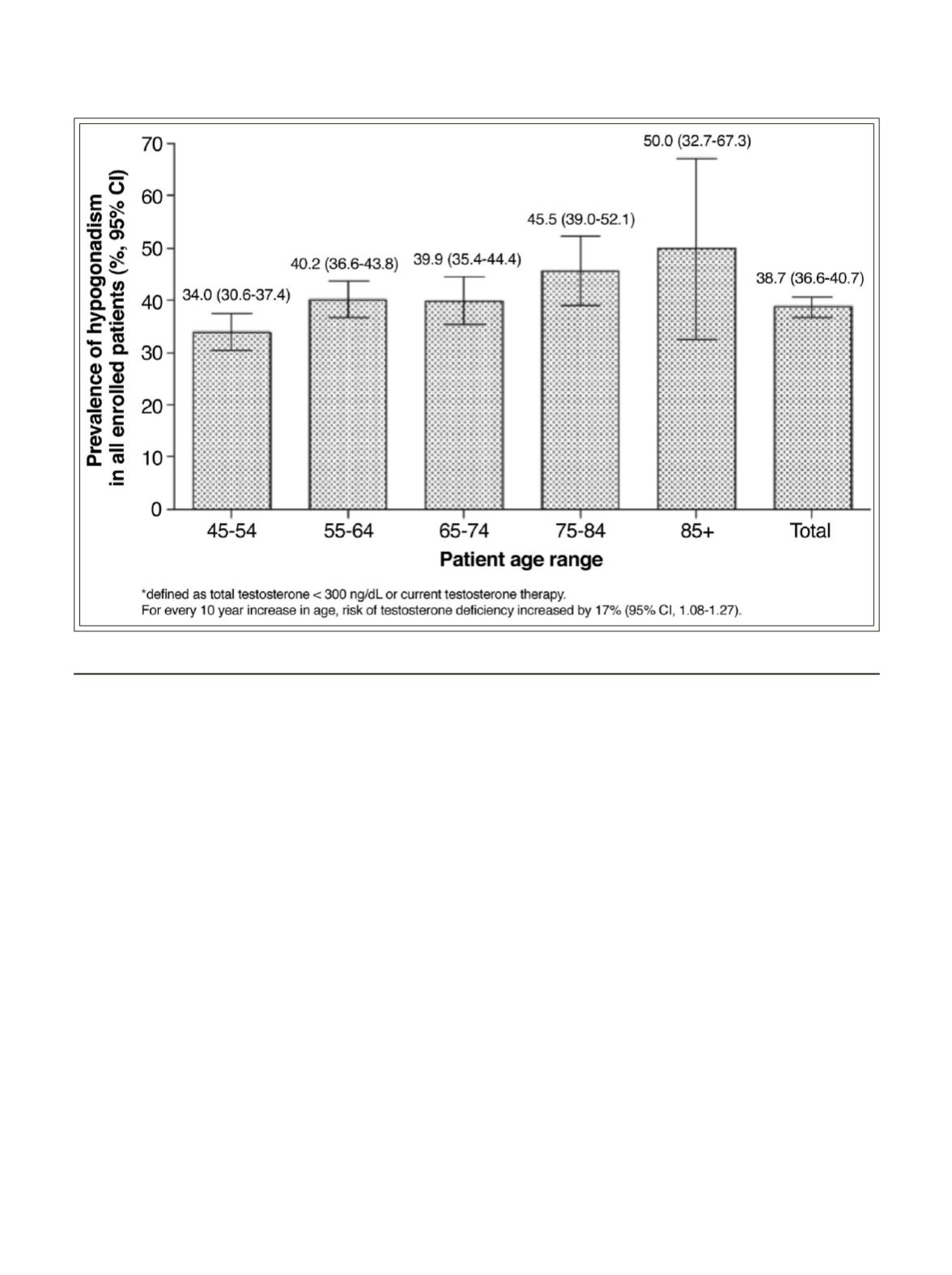
Figure 1.
Age-specific prevalence of biochemically defined testosterone deficiency*
15
41
Testosterone deficiency: myth, facts, and controversy


