Indexed in Index Medicus and Medline
Indexed in Index Medicus and MedlineIt has been reported that at least 30% of men over 50 have moderate benign prostatic hyperplasia (BPH).1 Oral medications are attractive, but symptom relief is modest as witnessed by International Prostate Symptom Score (IPSS) improvement. The incidence of side effects along with inadequate relief from the drugs prompt over 25% of men to discontinue treatment prematurely.2 If the lower urinary tract symptoms (LUTS) are particularly bothersome, the patients are tired of taking the medications, the medications fail or if the signs of urinary obstruction increase to the level that warrants prompt medical attention, surgical procedures are necessary.
Transurethral resection of the prostate (TURP) is considered the “gold standard” for BPH offering the best IPSS improvement.3 This improvement, however, comes with a 20% perioperative morbidity rate and potential long term complications including incontinence (3%), strictures (7%), erectile (10%) and ejaculatory (65%) dysfunction.4,5 New laser-based modalities have been developed to decrease bleeding when compared to TURP. Unfortunately, these newer ablative techniques still cause comparable postoperative and long term morbidity as the prostate heals.
The Prostatic Urethral Lift is described well in the literature.6-8 The UroLift (NeoTract Inc., Pleasanton CA, USA) implant holds the prostate lateral lobes apart improving the voiding channel and LUTS while minimizing exposure of the permanent implant to the urinary stream. The therapeutic effect of the Prostatic Urethral Lift appears to be considerably stronger than medical therapies, much faster acting and more predictable than thermal therapies and successfully avoids the morbidity and complications of TURP or laser therapies.3,7 There is minimal or no bleeding and virtually no retrograde ejaculation or incontinence. The implant procedure has been refined since its early description and we describe the preferred technique conducted using local anesthesia as an outpatient.
Patient
This minimally invasive therapy can yield excellent results if patients are properly selected. The Prostatic Urethral Lift is not a substitute for surgical ablation in patients experiencing urinary retention, possessing a decompensated urinary bladder or whose prostate size is over 100 cc. Cystoscopy and prostate ultrasound should be conducted to eliminate candidates who have large median lobes as this therapy has been designed for lateral lobe obstruction. While prostate sizes from 20 cc to 100 cc have been successfully treated, we recommend starting with prostates 50 cc or below to learn the technique. These glands will require fewer implants as the urologist learns the most efficient locations at which to retract the lateral lobes.
Anesthesia
The procedure has been successfully performed under general, spinal, or just local anesthesia with either no sedation or minimal oral or intravenous sedation. Because the ability to use a truly local anesthetic is a tremendous advantage of the UroLift system treatment when compared to other surgical modalities, it is useful to describe the preferred local anesthetic regimen.
All procedures we have performed in the recent randomized study were conducted using topical local anesthesia and oral sedation with the following protocol:
1) Oral anxiety drug (e.g. Valium) and anti-inflammatory (e.g. Celebrex or Motrin) 30 to 60 minutes in advance.
2) Catheterize and drain bladder and instill 20 cc of 2% lidocaine liquid chilled to 4oC. While removing the catheter, instill 20 cc chilled lidocaine gel into urethra.
3) Apply penile clamp for 20 minutes and rest the patient in sitting or lithotomy position.
Local anesthesia “tricks of the trade”
Experience has shown the most important component of local anesthesia is surgeon patience and communication. Adequate time must be given for the topical lidocaine and the preoperative sedation to take effect. Gentle and slow movements with the cystoscope while narrating to the patient allows for the easiest and best tolerated procedures. It is also helpful to have a patient support person at the head of the table to engage the patient in conversation. Discomfort is primarily from depression of the cystoscope necessary to cross the bladder neck at the beginning of the procedure. Deployment of the needle and implant appear to be well tolerated.
Equipment
The UroLift implant is a permanent implant consisting of a nitinol capsular tab (0.6 mm diameter X 8 mm long), a stainless steel urethral end piece (8 mm x 1 mm x 0.5 mm), and a size 0 polyethylene teraphthalate (PET) nonabsorbable monofilament, Figure 1. The UroLift system delivery device is pre-loaded with the implant and contains a spring-driven 19-gauge curved needle that reliably traverses prostates up to 100 cc6 thereby depositing the capsular tab of the implant onto the capsule. Direct visualization of implant placement is achieved using a 2.9 mm 0o telescope (Storz Ref# 10324A) inserted into the UroLift system which inserts into a 20F cystoscopy sheath (Storz Ref # 27027C). The number of UroLift implants required is typically four, but depends on prostate size and configuration. Key features of the small implant are that the urethral end piece invaginates into the prostate tissue to avoid encrustation, and that the monofilament is very easily thermally cut, allowing routine TURP or laser vaporization should it be desired at a later time.6
Surgical technique
Cystoscopy is conducted by gently advancing a standard 20F sheath to assess urethral condition, to rule out obstructive median lobe, assess degree of trebeculation and other obstructive sequelae, visualize the orifices and to plan implant placement. The sheath is then advanced into the bladder and the telescope bridge is replaced with the UroLift system. Actual delivery of the UroLift implant is achieved in a relatively straightforward manner by the following steps:
1) Unlock the needle safety lock.
2) Depress the needle trigger to fire the spring-loaded 19 gauge needle.
3) Retracting the needle leaves a tab on the prostate capsule attached to a monofilament that is tensioned by the device as the needle fully retracts. Interestingly, the device tailors the implant to the prostatic lobe at that location. Thus the length of each implant delivered varies between prostates and prostate locations.
4) Depress the release button to install a self-locking double walled urethral end piece onto the monofilament and trim the excess suture in a single step.
Tips and tricks of surgical technique
The operative technique goal is to create a continuous channel through the anterior prostatic fossa from bladder neck to veru montanum. Systematically, implants are delivered to both right and left lateral lobes advancing from approximately 1.5 cm distal to the bladder neck. After each set of implants the prostate is assessed cystoscopically; if a continuous channel is then observed, the procedure is deemed complete. The urethral mucosa can be quite fragile, and bleeding easily obscures vision. Care is taken throughout the positioning procedure to avoid trauma to the urothelium.
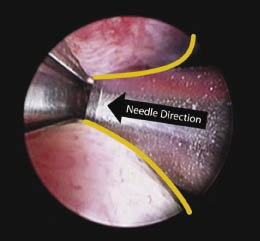
The UroLift delivery device moves easier and with less mucosal abrasion if it is turned 90 degrees to either side, and every effort is made not to rotate the device while within the prostatic fossa. Contact with the lateral lobes where the implants will be deployed is avoided until the operator has selected his target location. The lateral lobe is then compressed with the beak of the device and the implant deployed. Experience has shown the critical part of the prostate to treat is just distal to the bladder neck. With the device tip at the bladder neck, it is withdrawn under direct vision 1.5 cm and then pivoted laterally to approximately 20 degrees to 30 degrees from center. The compression point is in the top third (usually at the 2:30 and 9:30 position on the clock) of the lobe such that some tissue bulge occurs above but the majority below (posterior), thus forming a “B” shape, Figure 2.
What works
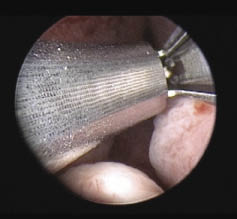
Once the prostatic urethra is expanded with a pair of implants just distal to the bladder neck, the prostate should be visualized from the veru montanum. In small, short prostates, one set of implants will complete the procedure resulting in a widely open prostatic fossa. Typically for a gland in the 40 cc-60 cc range, another pair of implants should be placed just anterior to the veru montanum. These distal implants should be deployed with the veru montanum in view and the device tip angled similarly to the initial implants, Figure 3.
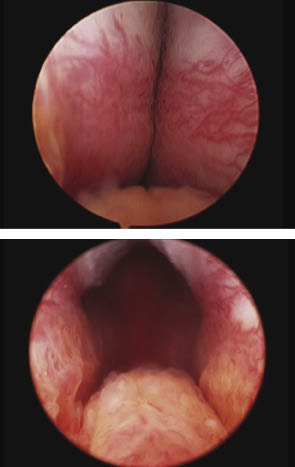
In prostates less than 60 cc, two to four implants typically open a continuous anterior channel. In larger prostates additional implants may be required between proximal and distal deployments. In larger prostates it should be appreciated that the goal is not necessarily to widely open the complete prostatic fossa, but to preferentially open a continuous channel through the anterior aspect of the prostate, Figure 4.
What doesn’t work
Experienced urologic surgeons accustomed to complete resection of the prostatic channel must appreciate that this is not a TURP. While in small prostates a widely open “TURP-like” fossa can be achieved with two or four implants, in larger prostates it is important to preferentially open a continuous anterior channel. Over the course of development of the Prostatic Urethral Lift, we have learned that the presence of a continuous defect in the apposing lobes offers acceptable and durable results in prostates up to 100 cc.6,7 As with many surgical procedures the enemy of a good result is often attempting to achieve a perfect result. With large lateral lobes placing implants below the anterior channel can potentially close areas of the newly created anterior channel.
The Prostatic Urethral Lift shows very promising performance in treating men whose quality of life is compromised by BPH/LUTS. The therapeutic goal of this procedure is to achieve maximal relief from symptoms with minimal recovery time. To achieve this goal, patient selection and technique are paramount. Unlike TURP or laser ablation the Prostatic Urethral Lift approach is to preserve the urethral mucosa and minimally disrupt the underlying tissue. It is this unique aspect of the procedure that allows for rapid relief from symptoms with minimal postoperative discomfort. We offer in this manuscript our preferred technique applied in over 50 patients to achieve the best results. Unlike prior technologies of minimally invasive treatment of BPH such as thermal therapies, Prostatic Urethral Lift patient outcomes can be optimized with superior surgical skill and decision-making.
The 2010 Canadian Urological Association4 and 2010 American Urological Association BPH guidelines5 recognize that TURP remains the benchmark for interventional BPH therapy. TURP is highly effective in improving symptoms and urodynamics and is associated with only a 15% retreatment rate over 8 years.4 While clearly effective in treating BPH, TURP is associated with a 20% morbidity rate including perioperative and intermittent postoperative bleeding, necessity for blood transfusions, TUR syndrome, necessity for prolonged catheterization and hospitalization, urinary incontinence, urethral strictures, erectile dysfunction and a very high retrograde ejaculation rate.4,5
BPH patients who have severe enough progression of their disease to present with urinary retention, decompensated bladders or deteriorated renal function should receive maximal surgical intervention, namely TURP or laser ablation. For the remaining vast majority of symptomatic men, BPH is a quality of life issue. With the goal to improve quality of life, patients and their physicians carefully weigh improving LUTS with the potential to compromise other body functions. Pharmacologic use demonstrates this well, as up to 30% of men taking BPH drugs discontinue therapy because the adverse effects outweigh the benefit.1,2 Of this large population of patients dissatisfied with medication, only a small proportion elect TURP as a next stage therapy. While clearly presenting an opportunity to relieve LUTS, TURP and laser vaporization represent significant risk to sexual function and, to a lesser extent, continence. Several studies have shown that LUTS has a smaller impact on overall quality of life than do sexual function or continence.9,10 Microwave and radiofrequency heating therapies indeed have fewer complications but they are associated with unpredictable results and 1-2 months of worsened symptoms before improvement.4,5
Clinical experience with this new treatment for BPH is encouraging. It can be done under local anesthesia as an outpatient and has been shown to result in a 40% mean improvement in both IPSS and urinary flow at 2 years. A remarkable advantage when compared to other interventional therapies is that patients report immediate improvement in symptomatology and a complete return to normal activity by 9 days. To date all patients studied report preservation of ejaculatory function and continence.7,8
The UroLift system is approved for sale in Canada and other countries for the treatment of symptoms due to urinary outflow obstruction secondary to BPH in men over the age of 50. In the United States, the UroLift system is currently being studied in a randomized controlled trial for the indication for the treatment of BPH. Study results are expected to be reported early next year. In Europe a post-market randomized study comparing UroLift system treatment to TURP is underway. With high quality clinical data emerging, this unique therapeutic offering may be shown to have a permanent place in our repertoire of care for BPH.
For most symptomatic men LUTS secondary to BPH is a quality of life issue. Treatment with the UroLift implant can be performed with local anesthetic as an outpatient. It has been shown to offer rapid relief of symptoms while maintaining normal prostate and sexual function. Ideal surgical technique can minimize postoperative adverse effects such as mild to moderate dysuria and hematuria and optimize effectiveness of this minimally invasive therapy. The UroLift system appears to offer a unique paradigm for the treatment of BPH in a significant proportion of men whose disease has not progressed to become life threatening or requiring surgical intervention.
Authors are investigators for the UroLift system.
Accepted for publication March 2012
Address correspondence to Dr. Jack Barkin, Humber River Regional Hospital, 404-960 Lawrence Avenue West, Toronto, Ontario M6A 3B5 Canada