Indexed in Index Medicus and Medline
Indexed in Index Medicus and MedlineIntroduction
Photoselective vaporization of the prostate (PVP) using the 532nm GreenLight laser (American Medical Systems, Minnetonka, MN, USA) has shown over its evolution to be equivalent to transurethral resection of the prostate (TURP), specifically for small to medium sized glands.1-13 Benefits of this modality include reduced complications, shorter hospitalization and catheterization as well as the ability to treat patients who are anticoagulated and with
coagulopathies.14,15
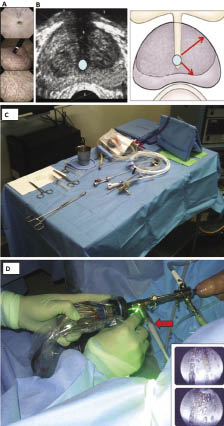
Since described by Malek et al using the potassium-titanyl-phosphate 80W system,16-17 there have been two significant upgrades in the laser device, namely the increased power with the use of lithium triborate, offered by the 120W HPS (2006) and the 180W XPS (2010) systems. Such increase in power output and improvement in laser beam collimation allow for more time-efficient tissue treatment. The second upgrade has been the new XPS-specific, MoXy liquid-cooled, steel-caped fiber provides significant improved speed and efficiency during vaporization by reducing tissue debris devitrification, Figure 1a. It is this principle of quartz-cap degradation on former fibers that significantly reduced power delivery throughout procedure. To achieve the proven safety profile of the GreenLight HPS system and improve the rate of vaporization, the power of the XPS/MoXy system was increased by 50% while simultaneously increasing the area of the laser beam by 50% (0.28 mm2 versus 0.44 mm2), Figure 1b, 1c, 1d. The benefit of the joint XPS system and MoXy fibre is a wider tissue vaporization effect without sacrificing the depth of vaporization and coagulation (< 2 mm). Compared to first and second generation systems, the latest XPS model significantly increases the speed of tissue removal (twice the speed of HPS) and durability of fiber longevity (often 1 fiber per case), Figure 1e, 1f, 1g.
Unfortunately, for the novice urologist embarking on GreenLight PVP, there has been a battery of published techniques using GreenLight for the treatment of benign prostatic hyperplasia (BPH).6 However, the ultimate outcome of any technique is thoroughness of prostatic tissue vaporization down to the surgical capsule. Herein, we present our approach that focuses on early identification of anatomic landmarks and systematic energy delivery.
Pre-op assessment of GreenLight XPS candidates
A thorough history and physical examination is essential to evaluate PVP candidates as suggested by both the American Urological Association (AUA) and Canadian Urological Association (CUA) BPH-guidelines. Use of the American Urological Association Symptom Index (AUA-SI) is an excellent, validated, quantitative assessment tool to evaluate symptoms and bother. A quantitative assessment of bother (as defined in the QoL question) is recommended to grade the severity of lower urinary tract symptoms (LUTS) and to understand the degree of bother caused by those symptoms. A focused physical examination should be performed to assess the suprapubic area for bladder distension, and motor and sensory function of the perineum and lower limbs. A digital rectal exam (DRE) should be performed to evaluate anal sphincter tone and the prostate gland with regard to approximate size, consistency, shape and abnormalities suggestive of prostate cancer. The DRE estimation of prostate volume has been shown to be inaccurate when compared to transrectal ultrasound (TRUS) and it for that reason, I recommend prostate sizing prior to intervention, Figure 2a. Not only does it properly optimize operative time planning, it also assists the anesthesia team with medication dosing, particularly with spinal anesthetics. Furthermore, prior to all interventions, urine flowmetry and post-void residual volumes are obtained to confirm bladder outlet obstruction. Flexible cystoscopy is also carried out to assess for the presence of any urethral pathology (stricture), prostatic length, lobe asymmetry or medial lobe presence and the condition of the bladder (trabeculation, diverticula, tumor or stones), Figure 2b. Serum prostate-specific antigen (PSA), urinalysis and urine culture are also obtained on all men prior to surgery.
Dedicated urodynamic study would only be suggested in a male patient with significant overactive bladder symptoms and neuropathic conditions (diabetes, disc herniation or upper neurological defects). A cystometrogram (CMG) would also help in the preoperative counseling of men with significant urinary retention (> 1 L) to assess detrusor contractility.
Informed consent is obtained with surgical risks discussed, which include:18-25 prolonged hematuria (> 2 weeks) (15%), irritative voiding symptoms (20%), urinary retention (5%) requiring replacement of Foley catheter, urinary incontinence (1%), retrograde ejaculation (> 70%), urinary track infection (3%) as well as the rare possible injury of the bladder and ureteral orifices.
Set up and equipment
Unless medically indicated (anticoagulated male, significant medical comorbidity), GreenLight XPS procedures are carried out at our institution as same-day, outpatient surgery. General anesthesia with laryngeal mask or a spinal anesthesia with a short acting medication (chlorpromazine) is preferred since it favors successful catheter removal 4-6 hours following surgery.
Before procedure initiation, we suggest that the surgeon verify all equipment is set up (camera attached to working sheath, white balance, light cord and irrigation tube positioned) and back-table material (catheter placed over stylet and syringe with 30 cc NS) ready before initial cystoscopy, Figure 2c. That way, there will be less unnecessary scope movement within the patient, thereby reducing unwanted bleeding. We utilize a Storz 24Fr laser resectoscope and assess the condition of metallic edges as part of our checklist. Room temperature 3 L normal saline bags are hung through a Y-tube adapter 60 cm-80 cm above patient height. Furthermore, the MoXy fiber is cooled via a dedicated 1 L bag of saline. The patient is prepped with a disinfectant solution (chlorhexidine 4%) and put into the dorsal lithotomy. Preoperative antibiotics and if indicated, subcutaneous heparin are administered. We also suggest for those starting on their learning curve to digitally record initial cases for self-evaluation and teaching purposes.
Surgical mechanics of TURP versus GreenLight XPS
Compared to standard TURP, which is dominantly a one-handed procedure, GreenLight PVP demands a greater deal of two-hand involvement.17-25 More specifically, the non-dominant hand stabilizes sheath at verumontanum, the dominant hand extends the loop to the bladder neck and within 2-3 seconds, supinates the wrist to excise a strip of tissue. Depth of loop penetration is not visually guided and is controlled with the non-dominant hand and gauged by surgeon experience. With GreenLight XPS, there is more dependence on two-hand coordination to achieve optimal results. As such, for the new user, GreenLight XPS poses a mechanically more complex and different approached procedure. Rather than remaining stationary at the verumontanum, the non-dominant hand, which holds the camera, is withdrawn simultaneously as the MoXy fiber is pulled back during vaporization. This ensures a safe working distance with the laser energy so as not to damage the metal sheath or camera lens. The non-dominant hand is also responsible for maintaining optimal treatment distance (1 mm-3 mm) from the tissue. As such, the non-dominant hand is much more dynamic throughout the procedure; as is the dominant surgeon hand. Compared to the TURP, which the mechanics is in the turn of the wrist, the GreenLight XPS technique involves the coordination of movements at the wrist, elbow and shoulder.
Factors influencing vaporization efficiency
Working distance
The rate of efficiency of laser treatment declines after 3 mm, and so I try to work 1 MoXy fiber cap (width = 1.8 mm) away from the prostate surface, Figure 1f.
Energy settings
When treating the prostatic urethral mucosal surface, which is highly vascular, initial setting should be 80W for vaporization and 30W for coagulation. Once the mucosa has been treated and the adenoma is exposed with a larger working space, the vapor setting is increased by increments of 10W up to 120W and for larger glands
(> 80 g) and more fibrous tissue, increased to 180W.
Sweep speed and angle
Based on bovine models, a sweep speed of 0.5 to 1.0 sweeps/second has been demonstrated to be more efficient and remove significantly more tissue than faster sweep speeds.19 Therefore, in our clinical practice we conform to the above mentioned sweep speed during prostate resection (2 seconds per each 30-degree rotation or 4 mm sweep per second). Compared to conventional TURP, the surgeon must show patience and not sweep at faster rates. Ex-vivo analysis has showed that larger sweeping angles generated wider but more superficial vaporization defects, leading to smaller vaporized volumes. Specifically, vaporization volumes with angles of 0, 15, or 30 degrees were significantly greater than those with rotational angles of 45, 60, and 90 degrees.20
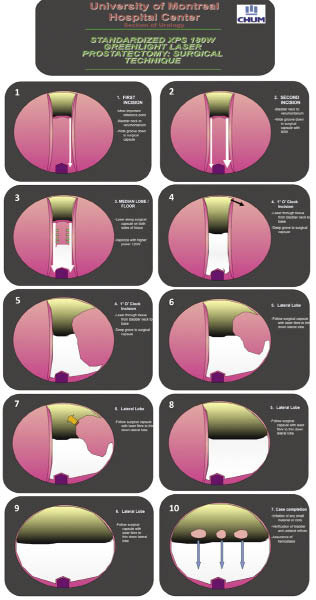
Greenlight XPS procedure description, Figure 3
STEP 1: Getting started and landmark demarcation
Careful, atraumatic, camerascopic introduction of the working sheath is essential to avoid unnecessary mucosal bleeding, particularly at the bladder neck and median lobe. The bladder should be inspected for tumors as well as identification of the orifices especially in the case of high bladder necks. In cases with large median lobes, I will avoid excessive torqueing and occasionally defer identification of ureteral orifices until the bladder neck has been debulked. Careless bleeding will slow down tissue treatment and hamper visual acuity.
I routinely mark the limits of dissection from the 3- to 9-‘clock locations at both bladder neck and apex using the 30W coagulation setting. This maneuver limits bleeding and allows for a visual guide to avoid migration of treatment beyond the verumontanum.
I also leave the last 1 cm just behind the verumontanum untreated and manage this just prior to case completion with lowered energy setting.
Planning the initial incision depends on the size and dimensions of the gland. High bladder necks and particularly, kissing lateral lobes often require debulking to allow for adequate working space. For small sized glands (< 60 g), an initial treatment groove down to the capsule is made at 5 o’clock from the bladder neck to the verumontanum at 80W power. This initial incision, which I feel is extremely valuable, serves as a depth reference throughout the procedure. For larger glands (> 60 g) or those men with median lobes, a second grooved-incision is created at the 7 o’clock positions prior to clearing the floor.
STEP 2: Prostate floor tissue treatment
Once the initial grooves are made, the floor is then treated at either 120W or 180W. The key during this surgical segment is to treat tissue with the laser fiber cap in contact with the capsule however rotating the cap and delivering energy horizontally along-side the capsular fibers. We feel that this helps reduce the unlikely chances of capsular perforation and more clinically-relevant, urinary irritative symptoms. Occasionally, fibrous and avascular tissue can be encountered which does not vaporize well. In such instances, the tissue can be enucleated from beneath along the capsule and released into the bladder for later removal. The surgeon should be cognizant of the width of the tissue strip to allow facile removal.
STEP 3: Lateral lobe treatment
Once the floor and median lobe have been treated (5- to 7- o’clock zone), I generally turn my attention first (being a right-handed surgeon) to the patient’s left lateral lobe. With the working sheath rotated by tilting the light cord and therefore the 30-degree cystoscope lens to a 9-o’clock position in my hands (thereby avoiding direct laser firing at the metal beak), another groove is treated at the patient’s 1-o’clock prostate tissue, Figure 2d. This is taken down repetitively to the capsule to allow the bulk of the left lobe to drop into the urethral canal. The surgeon can then treat the pedicle of tissue from the 5- and 1-o’clock positions by side firing again at the tissue from the level of the capsule. I find the 180W power setting shows its great advantage during lateral lobe treatment. Formerly with the HPS 120W system, I would incise long pillars of tissue and free them into the bladder to optimize OR time however with the higher power setting, the GreenLight XPS obviates the need for tissue enucleation. Once complete, the high-release grooved incision is made at the 11-o’clock area to drop the patient’s right lobe and thereafter treat with systematic vaporization.
STEP 4: Managing bleeding
Occasionally, arterial bleeding is encountered during tissue vaporization, which significantly obscures vision. I will usually shorten my working distance with the laser fiber to optimize water flow and use the beak of the sheet to compress the bleeding vessel. Once visualized, the aiming beam of the laser is aimed and the vessel is circumscribed using the 30W coagulation setting. For instances where proximal tissue obscures the location of the vessel, tissue vaporization can be performed to expose the bleeding area. Vaporization over the bleeding area with a larger working area and faster sweep speed can also be attempted to coagulate the bleeder.
In the instance where the above measures are not satisfactory for hemostasis, I will use a Bugbee electrode to control the vessel in an end-on manner. Another option is to suspend laser surgery and place a 20F catheter with 30 mL in the balloon and provide 5 minutes of manual traction prior to resuming the procedure.
STEP 5: Apical treatment
Careful attention should be taken to the apex. The power should be lowered to 80W to avoid thermal sphincteric trauma. I will occasionally try to leave a small flap of apical tissue just above the verumontanum for younger men who desire antegrade ejaculation and older gentlemen (> 70) for risk of stress urinary incontinence.
STEP 6: Assurance of tissue treatment, hemostasis and case completion
Upon procedure completion, I will first empty 50% of the bladder and replace the scope back into the sheath with the water flow reduced to a minimum. Aside from small venous oozing areas commonly along the bladder neck floor and mucosal edges at the apex, which are easily coagulated with the 30W TruCoag setting, arterial pumpers are sought and treated. If the transitional zone tissue has been adequately treated, the cavity will remain a large defect. I again like to assess the bladder wall, ureteral orifices and identify any tissue pieces which can be removed. The bladder is then filled before passing the 2-way 20F urinary catheter over a stylet guide. Thirty milliliters of saline are instilled to fill the balloon. I generally rinse the bladder again with the saline irrigation to remove tissue pieces or any small clots which could obstruct the catheter.
In the occasional instances where the outflow is bloody, Foley traction can be provided for 5 minutes while irrigating the bladder. For men who were treated while in an anticoagulated state (ie. Coumadin for a metallic heart valve), I will place a 22F 3-way catheter and plug the inflow port in the event continuous flow is required. These men are kept at least overnight for observation.
Postoperative management
After transfer to the recovery room, the patient is hydrated through an intravenous and encouraged to drink fluids. Six hours following the procedure, the patient is evaluated for a trial of void (TOV). Factors that affect attempting TOV include the color of urine, time of the day, type of anesthesia and status of the bladder. The bladder is filled with 300 mL of saline and a bladder scan residual volume is obtained prior to discharge. Discharge medications include a fluoroquinolone (Ciprofloxacin) for 7 days and a stool softener to avoid constipation. Men are encouraged to avoid narcotics for discomfort. Patients are advised to avoid any strenuous activity, Vasalva-like maneuvers (heavy lifting > 20 lbs) including sexual activity for 2-3 weeks, especially those who resume anticoagulation. If anticoagulation medication was stopped before the procedure, it would be restarted following recommendations from the internist. If anticoagulants were not stopped, the high risk patient would be observed in hospital for 24-48 hours.
Follow up
A scheduled appointment is organized 1 month after hospital discharge. In our experience 20%-30% of patients will report irritative urinary symptoms (frequency, terminal dysuria), which tends to be self-limited. It is our practice to start men with severe symptoms on an antimuscarinic agent and anti-inflammatories for 1-3 months and schedule a close follow up in clinic to re-evaluate their symptoms.
At 3 months a PSA, urinary flow rate and AUA-SI questionnaire (IPSS) is obtained to evaluate resolution of bladder outlet obstruction. A drop of at least 50%-70% in preoperative PSA should be expected following the intervention to verify the degree of adenoma removal.20 Given my interest in the clinical outcomes of such patients, follow up visits are also scheduled at 6 and 12 months followed by yearly assessments to assess the durability of GreenLight XPS.
Training recommendations
Until the GreenLight simulator along with universal physician laser-credentialing pathways exists, the training recommendations with the GreenLight XPS are dependent on whether the surgeon is an experienced or inexperienced user. For the experienced GreenLight user (one who has completed 30 cases) mentoring and proctoring should take place on at least one occasion. Coupled to the online training module, this will ensure the hands-on review new XPS features (increased power options (120-180W), TruCoag and FiberLife features) and equipment set up (internal fiber cooling).
The inexperienced PVP user who is a trained urologist should undertake a formal training course, complete the online new-users on-line training module, watch several (5-10) live procedures performed by an experienced surgeon, and be subsequently proctored for a minimum of five cases, although this number may vary depending on proctor’s discretion. Any supplemental, ongoing training should be conducted with the aid of the proctor. During the first 20 independent cases, the learning objectives should solidify the knowledge of prostatic anatomy, laser-tissue interaction (sweep speed, power setting and distance from tissue), standardized approach to the procedure and management of bleeding and complications.
Keys to success
Initial GreenLight XPS cases should be well selected and be properly screened with cystoscopy and TRUS. Uncomplicated men (no anticoagulation) with prostates sized less than 60 cc by ultrasonography, no median lobe are to be done at first. Personal experience suggests that it is poor patient selection (underestimating prostate volume only with DRE, presence of an unseen median lobe) that results in difficult working situations (little working space, bleeding) that drives surgeons back to their comfort zone being TURP. Another inexpensive tool that aids in surgeon education is the digital video recorder. There is tremendous value in self critique and peer evaluation.
Conclusion
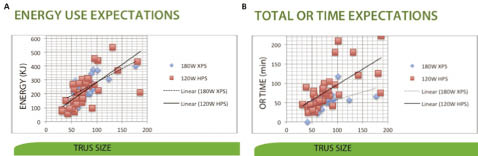
Since performing my first GreenLight XPS laser PVP procedure in April 2011, I have been able to treat over 100 men thus far ranging from 43 g to 229 g. It is my experience that the XPS system along with durability of the MoXy fiber, afford the urologist an effective treatment option for BPH however with shorter length of stay in hospital, less postoperative catheter time and the elimination of TURP syndrome electrolyte anomalies, OR time constrains and need for transfusion. From a cost perspective (approximately 800$ CAD per fiber), we routinely only use 1 fiber per case. I have had no fiber failure during treatment thus far with the MoXy fiber. With the GreenLight XPS system, I am able to complete 6-8 cases per surgical day and have impressively been able to treat larger glands with significantly quicker operative times, Figure 4,
without compromise of outcomes or increased complication. We are currently analyzing our first 100 XPS system patients and will be publishing our data shortly.
Disclosure
Dr. Kevin C. Zorn - American Medical System (AMS) –
consultant, proctor; Dr. Daniel Liberman - none