Welcome to the CJU website »
LOG IN

 Indexed in Index Medicus and Medline
Indexed in Index Medicus and Medline
Free Articles
HOWIDOIT
Olympus PlasmaButton transurethral vaporization technique for benign prostatic hyperplasia
Michael McClelland Jr, MD
Urology Austin, Austin, Texas, USA
MCCLELLAND M JR. Olympus PlasmaButton transurethral vaporization technique for benign prostatic hyperplasia. The Canadian Journal of Urology. 2011;18(2):5630-5633.
Objective: This article will describe an efficient and effective method of using Olympus PlasmaButton (Olympus, Southborough, MA, USA) for transurethral vaporizations of the prostate (TUVP).
Methods: This method was developed over the last 18 months. Patients undergoing this Olympus PlasmaButton TUVP had the inner aspect of the prostate vaporized until it was believed to be significantly open and unobstructed.
Results: Patients were found to do very well with what appears to be durable results. Postoperative short and long term bleeding has not been a significant issue using this method.
Conclusion: The Olympus PlasmaButton procedure is a new minimally invasive therapy for benign prostatic hyperplasia (BPH). As with all new technologies there are methods that a surgeon learns with increased experience that help make the procedure more effective, efficient, and safer. This article shows one surgeon’s technique that has been developed over time and has become a successful way to manage patients undergoing the minimally invasive transurethral vaporization of the prostate. There are probably other vaporization techniques that surgeons have learned with use of the PlasmaButton that may be equally effective.
Key Words: benign prostatic hyperplasia, transurethral vaporization of the prostate,
technique
Introduction
Surgical management of the prostate is still one of the most widely used, and effective methods to treat obstructive benign prostatic hyperplasia (BPH) symptoms.1 Over the last decade the surgical treatment for BPH has changed dramatically as new technologies become increasingly used in both private and teaching facilities. These new techniques have become safer, more efficient, and cost effective leading to their increased usage. As the technologies advance, new modalities and techniques for use of those modalities have evolved.
The Olympus PlasmaButton is one of the newest technologies for surgical management of BPH. It consists of a bipolar generator and button shaped electrode that uses saline for irrigation and can effectively vaporize large amounts of tissue in an outpatient setting, leading to improvement in lower urinary tract symptoms caused by BPH. Like all new technologies, there are certain steps that can improve both the efficacy and the efficiency of the procedure. Herein is described a set of techniques, developed from doing over 100 of these procedures by a single surgeon, that have been found to improve efficacy, efficiency, and overall patient outcomes.
Technique
Start of the procedure
Once the appropriate patient has been worked up and has consented to the procedure, a continuous flow resectoscope is then placed transurethrally using a visual obturator into the prostatic urethra. Inspection of the anatomy is done making sure to visualize the ureteral orifices and verumontanum, Figure 1. The working element is placed into the continuous flow sheath, and vaporization is begun at the bladder neck between the 4 o’clock position and the 8 o’clock position back to the level of the verumontanum. Care is taken to ensure that the verumontanum and the ureteral orifices are not damaged during vaporization.
Plasma vaporization therapy
The procedure for vaporization is simple. The generator automatically sets the default settings for cut and coagulation, both of which are controlled using a foot pedal. Variations to the standard settings have not been needed. Operating room staff education is minimal and has been taken care of by the Olympus/ACMI representative prior to the first case. Long deep strokes with the PlasmaButton lead to large amounts of tissue being vaporized in a short period of time, Figure 2. Care must be taken to make sure that direct visualization of the PlasmaButton is maintained at all times to ensure no damage is done to the ureteral orifices, verumontanum, and/or external sphincter. Vaporization may be safely done in both the forward and backward motions of the PlasmaButton which further increases the efficiency of the procedure. Once adequate vaporization has been performed on the posterior aspect of the prostate, the lateral lobes are then vaporized again starting at the bladder neck and working back to the level of the verumontanum, but not beyond to ensure no damage is done to the external sphincter. If any anterior tissue needs to be vaporized it is then done after the lateral lobes have been dealt with.
Hemostasis
Hemostasis with the PlasmaButton is usually much better than is seen with a bipolar transurethral loop resection of the prostate, and similar to that of the currently marketed lasers. When a bleeding vessel is seen it can usually be cauterized using the coagulation mode at the time of visualization. The coagulation technique is to apply pressure to the tissue while activating the coagulation mode until the tissue changes color and hemostatis is achieved. If the vessel is in an area that requires more treatment, then continued vaporization in that area can be performed until the desired depth of tissue removal is achieved. If the vessel is still bleeding after the continued vaporization, then cauterization is used for adequate hemostasis. Some physicians will use continuous suction on the outflow port of the continuous flow sheath. This surgeon has not noticed any benefit in visualization from this method, since visualization is usually excellent when bleeding vessels are cauterized as they appear.
Finishing the case
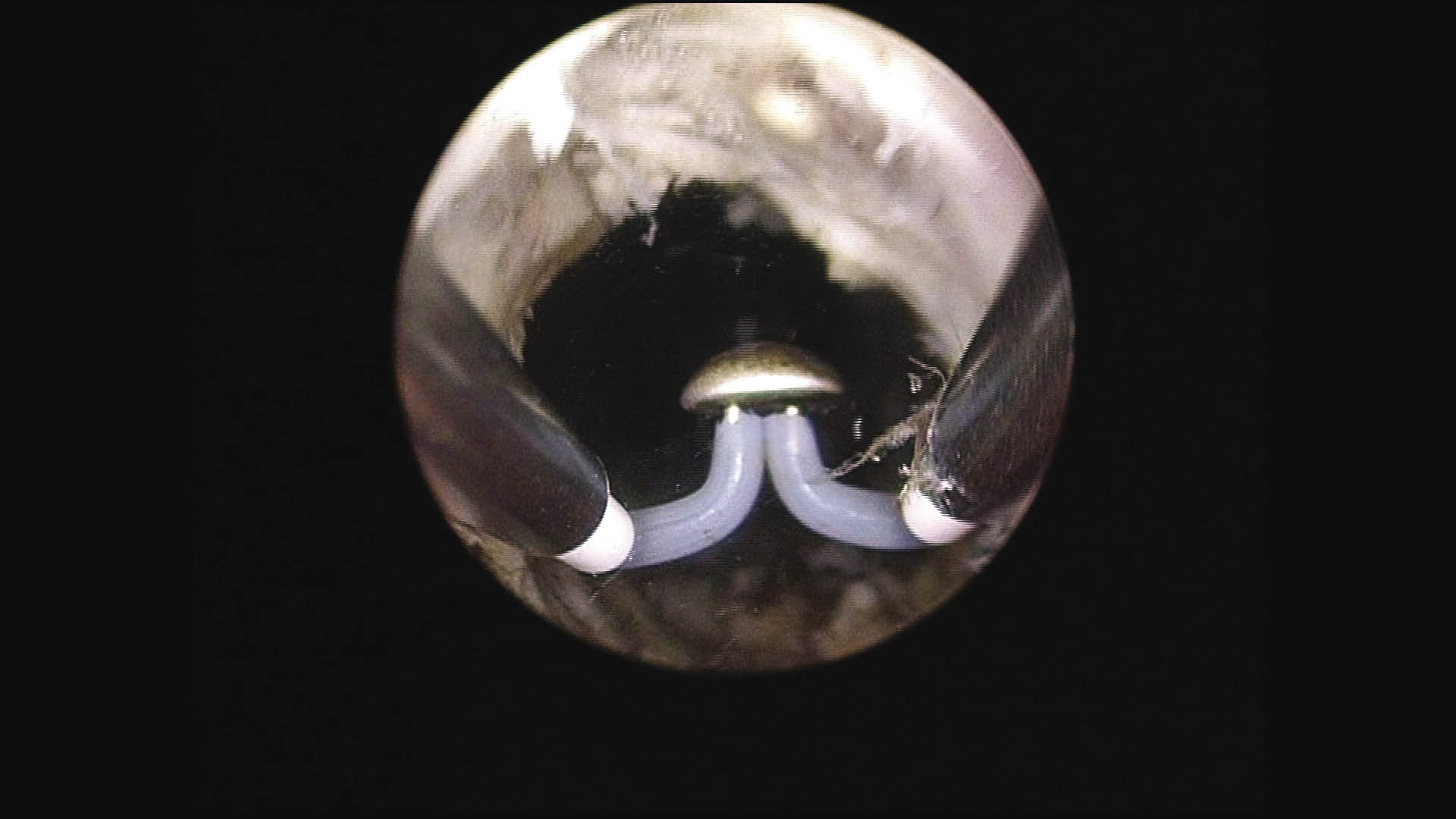
After achieving a wide open prostatic urethra, Figure 3, circular fibers of the capsule are sometimes seen indicating good depth of vaporization. Once a surgeon thinks enough tissue has been resected, decompression of the bladder by draining the irrigation fluid should be done with immediate reinsertion of the working element. At this time, turn on the irrigation fluid again and see if there are any bleeding vessels or tissue that still needs to be resected. This process is repeated multiple times until there are no other bleeding vessels and there is a wide open prostatic urethra with a decompressed bladder. It is common to repeat this step 3-5 times or more to ensure excellent hemostasis and patient outcomes.
Postoperative
At the end of the procedure a 24Fr 3 way Foley catheter is placed and manually irrigated until the irrigation fluid is clear and unobstructed by sediment. The patient is then transferred to the recovery room with continuous normal saline irrigation for 1 hour and then discharged home with a Foley catheter in place overnight in most cases. Patients are then instructed to remove the Foley at home on the following morning and call if they are having problems emptying their bladder. Patients who were in retention or had other underlying bladder pathology preoperatively will usually have the catheter for 2 to 7 days prior to a voiding trial.
Discussion
As more minimally invasive techniques have evolved in the treatment of BPH, safer, more effective and efficient technologies have allowed more patients to undergo surgical procedures to improve their voiding symptoms. The Olympus PlasmaButton vaporization is performed using normal saline allowing an increased amount of resection/vaporization without the fear of hyponatremia. The decreased bleeding and relatively short operative times make this an excellent outpatient procedure commonly performed in surgical centers. With the larger surface area of vaporization compared to other minimally invasive modalities, operative times should be less. Because of the efficiency of the Olympus PlasmaButton, larger glands that previously may have required a suprapubic prostatectomy may be effectively vaporized with an outpatient PlasmaButton procedure. Vaporization is done in a similar fashion to the transurethral resection of the prostate (TURP) approach, and may vary based on different physicians’ techniques. This article depicts a single surgeon’s approach that has been successful and efficient for both the patient and the surgeon. Preoperative instruction and teaching is similar to other transurethral resection type procedures. Great care is taken to let patients know that the symptoms will not be as optimal as they would like immediately postoperative. It is important to stress that there is a recovery time necessary for healing before the typical postoperative irritative symptoms have resolved. This time period is usually 2 to 8 weeks and the irritative symptoms can be minimized with anticholinergic medications used over the first 2 weeks.
One of the more common initial postoperative concerns is bleeding. Some physicians have experienced postoperative bleeding either immediately or days to weeks later. This can be minimized by emptying and decompressing the bladder towards the end of the procedure. Commonly when this is done and the surgeon looks back in the decompressed bladder, there will be vessels that need to be cauterized and/or more tissue that needs to be vaporized. Repeating this process until there are no other bleeding vessels and there is a wide open prostatic urethra has almost eliminated the postoperative bleeding issue and hopefully improved patients’ long term success.
Excessive use of the coagulation mode or “blanket coagulation” at the end of the procedure is not necessary. Coagulation of this type may actually increase the risk of delayed postoperative bleeding. Excessive use of the coagulation mode is theorized to increase sloughing weeks later leading to possible delayed bleeding. Instead, as mentioned previously, spot coagulation of specific bleeding vessels with bladder decompression is very effective at hemostasis and may lead to decreased risks of delayed bleeding.
Catheterization time is variable based on other physicians. In most cases patients can be catheter free in 1-2 days. Usually patients will receive continuous bladder irrigation in the recovery room for 1 hour, and then the patient is sent home with a Foley catheter overnight. Patients are then instructed to remove their Foley catheter the following morning at home and call if they are unable to void. Very few patients need repeat catheterizations with this method, and if they do, it only requires a simple nurse visit for a bladder scan and Foley catheter during normal business hours. Patients who had retention preoperatively tend to need a Foley catheter for a longer period. In those patients with preoperative retention, an initial voiding trial is usually done 3-5 days later rather than postoperative day number one.
There have been no studies to this author’s knowledge looking at the feasibility of the bipolar Olympus PlasmaButton TUVP in anticoagulated patients. Also, since the patient is not grounded for this procedure, there is no concern operating on patients with pacemakers.2 If the surgeon elects to resect tissue for a pathologic specimen, then there would be the same pacemaker issues as with any other monopolar procedure. If a physician thinks a biopsy of the tissue is necessary, then monopolar or bipolar loop resection could be done at any time during the PlasmaButton TUVP.3 Alternately, a physician may want to consider an in office transrectal ultrasound and biopsy prior to the PlasmaButton TUVP if indicated. As mentioned in the materials and methods, safety must always be considered. Direct visualization of the tissue being vaporized must be maintained at all times. Visualization of circular fibers can indicate the final extent of resection in that area. Other times visualization of these fibers may not be possible. That is where the decompression of the bladder towards the end of the procedure helps the surgeon realize when there has been enough vaporization for a good outcome. If there is still a significant amount of tissue falling into the prostatic urethra when the bladder is decompressed, more vaporization in that area should be done until there is a wide open prostatic urethra without any obvious bleeding vessels.
Conclusion
The Olympus PlasmaButton procedure is a new minimally invasive therapy for BPH. As with all new technologies there are methods that a surgeon learns with increased experience that help make the procedure more effective, efficient, and safer. This article shows one surgeon’s technique that has been developed over time and has become a successful way to manage patients undergoing the minimally invasive transurethral vaporization of the prostate. There are probably other vaporization techniques that surgeons have learned with use of the PlasmaButton that may be equally effective.
Disclosure
Dr. McClelland would like to disclose that he is paid by Olympus/Gyrus ACMI for consulting services and has received financial support from Olympus/Gyrus ACMI related to this article.
Accepted for publication March 2011
Address correspondence to Dr. Michael McClelland Jr., Austin Urology, 3100 Red River, Austin, Texas 78705 USA
Figure 1. Start of the case. Image of the untreated prostate.
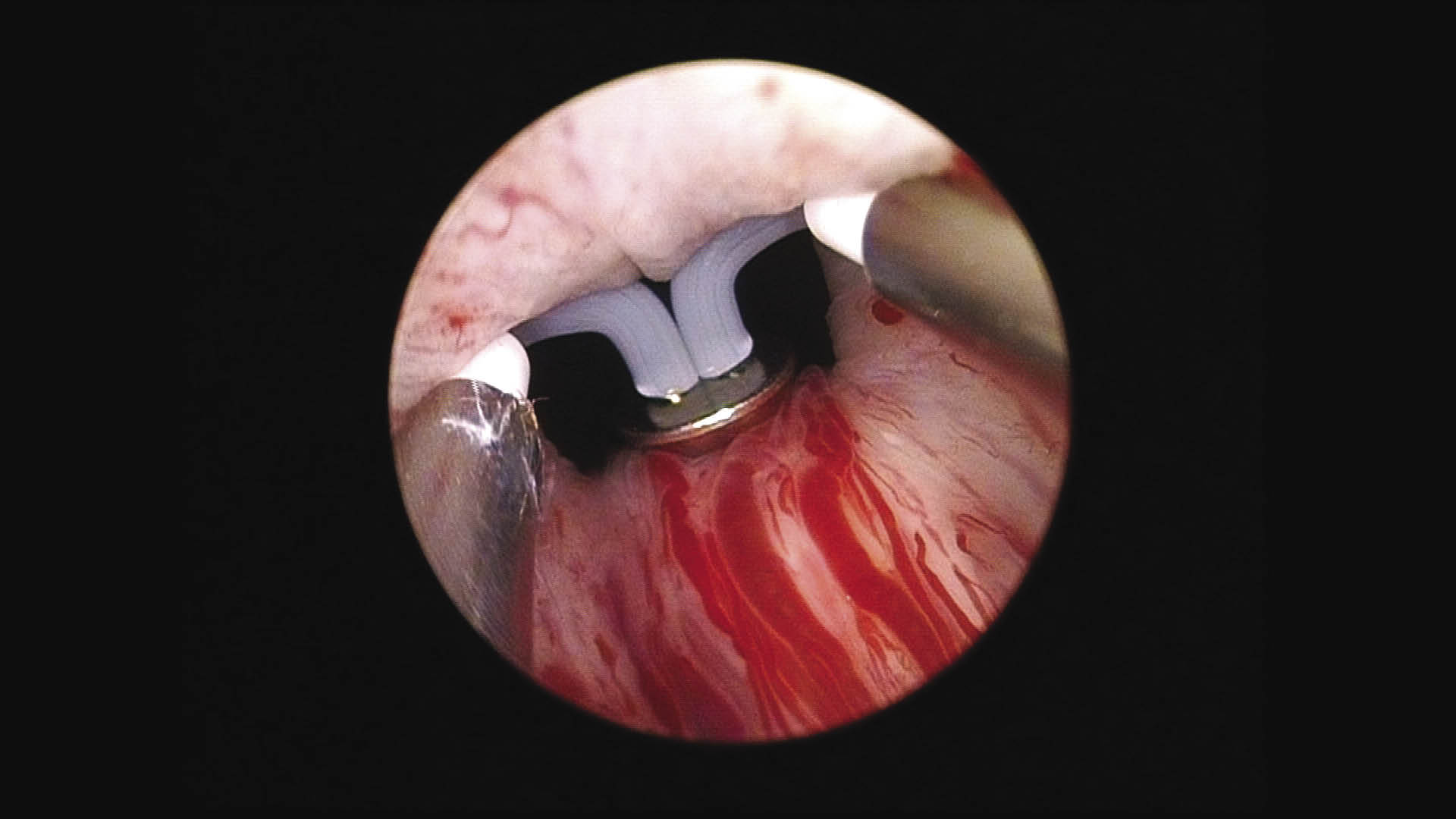
Figure 2. Early vaporization on the median lobe. Image of the PlasmaButton corona.
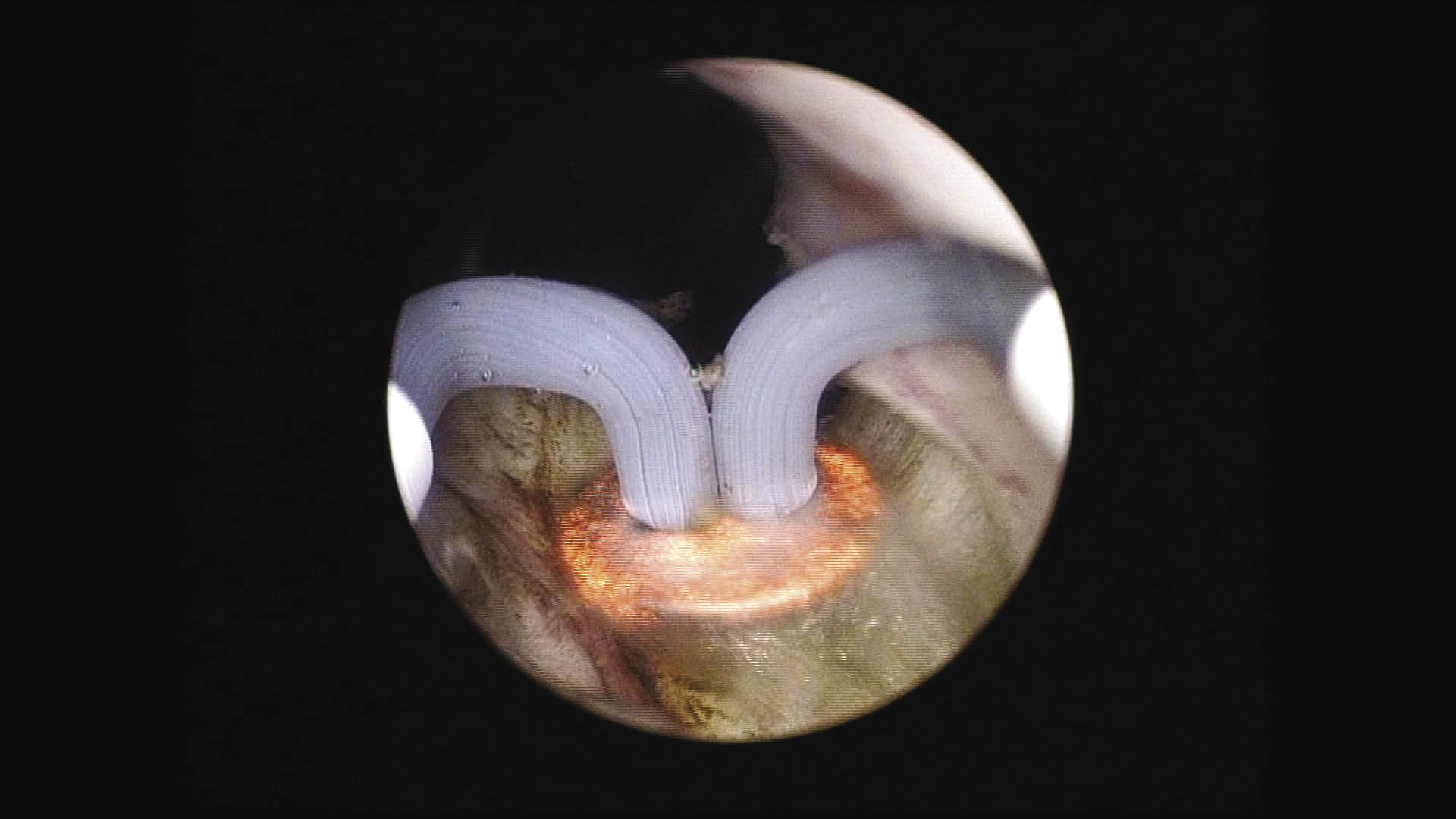
Figure 3. End of the case. Image of the treated prostate showing the prostatic opening.
References
1. Smith RD, Patel A. Transurethral resection of the prostate revisited and updated. Curr Opin Urol 2011;21(1):36-41.
2. Chen Q, Zhang L, Fan QL, Zhou J, Peng YB, Wang Z. Bipolar transurethral resection in saline vs traditional monopolar resection of the prostate: results of a randomized trial with a 2-year follow-up. BJU Int 2010;106(9):1339-1343.
3. Dellavedova T, Ponzano R, Racca L, Minuzzi F, Dominguez M. Prostate cancer as incidental finding in transurethral resection. Arch Esp Urol 2010;63(10):855-861.
Current Issue
December 2024, Vol.31 No.6