© The Canadian Journal of Urology™; 21(Supplement 2); June 2014
based on the FRS or the 2013 ASCVD risk calculator:
a thorough history; physical examination (including
measures of visceral adiposity); assessment of ED
severity and duration; evaluation of fasting plasma
glucose; resting electrocardiogram; serum creatinine
(estimated glomerular filtration rate) and albumin;
creatinine ratio; and presence or absence of other
features of the Met S.
12,13
Based on results of the aforementioned assessments,
the physician may encourage lifestyle changes which
are likely to reduce CVS risk and improve erectile
function.
51,52
Pharmacotherapy to control specific CVS
risk factors (eg, hypertension, diabetes, hyperlipidemia)
may also be appropriate. Menwho appear to be at high
risk for CVS events should be referred to a cardiologist.
We suggest that intermediate risk men (per FRS or
2013 Risk Calculator defined as low 10 year ASCVD
risk but high lifetime ASCVD risk) with vasculogenic
ED and no overt CVD undergo further noninvasive
evaluation of CVS risk using exercise stress testing
(EST) to exclude obstructive disease, carotid intima-
media thickness (CIMT), ankle-brachial index (ABI), or
suggest that this tool may be particularly helpful in
identifying silent CAD inmenwith EDanddiabetes.
53,54
Carotid intima media thickness (CIMT)
Although the value of CIMT has not been evaluated in
men with ED, ACCF/AHA,
53
and more emphatically,
the Society forHeartAttack Prevention and Eradication
(SHAPE) task force,
55
assert that it is reasonable to
perform CIMT assessment during evaluation of
intermediate risk patients. Studies published since
these guidelines were developed support the value
of this methodology in CVS risk assessment. In an
evaluation of 441 asymptomatic subjects < 65 years of
age (mean age, 50 years ± 8 years) with no history of
CAD or diabetes, Eleid et al
56
reported that 38% of the
336 subjects deemed low risk based on the FRS had
high risk carotid ultrasound findings (ie, CIMT ≥ 75
th
percentile adjusted for age, sex, and race or presence
of plaque). Similarly, Naqvi et al
57
found that 50%
of 136 asymptomatic subjects (mean age, 57 years ±
11 years) with no history of vascular events and FRS
< 10% had CIMTs ≥ 75
th
percentile. However, Den
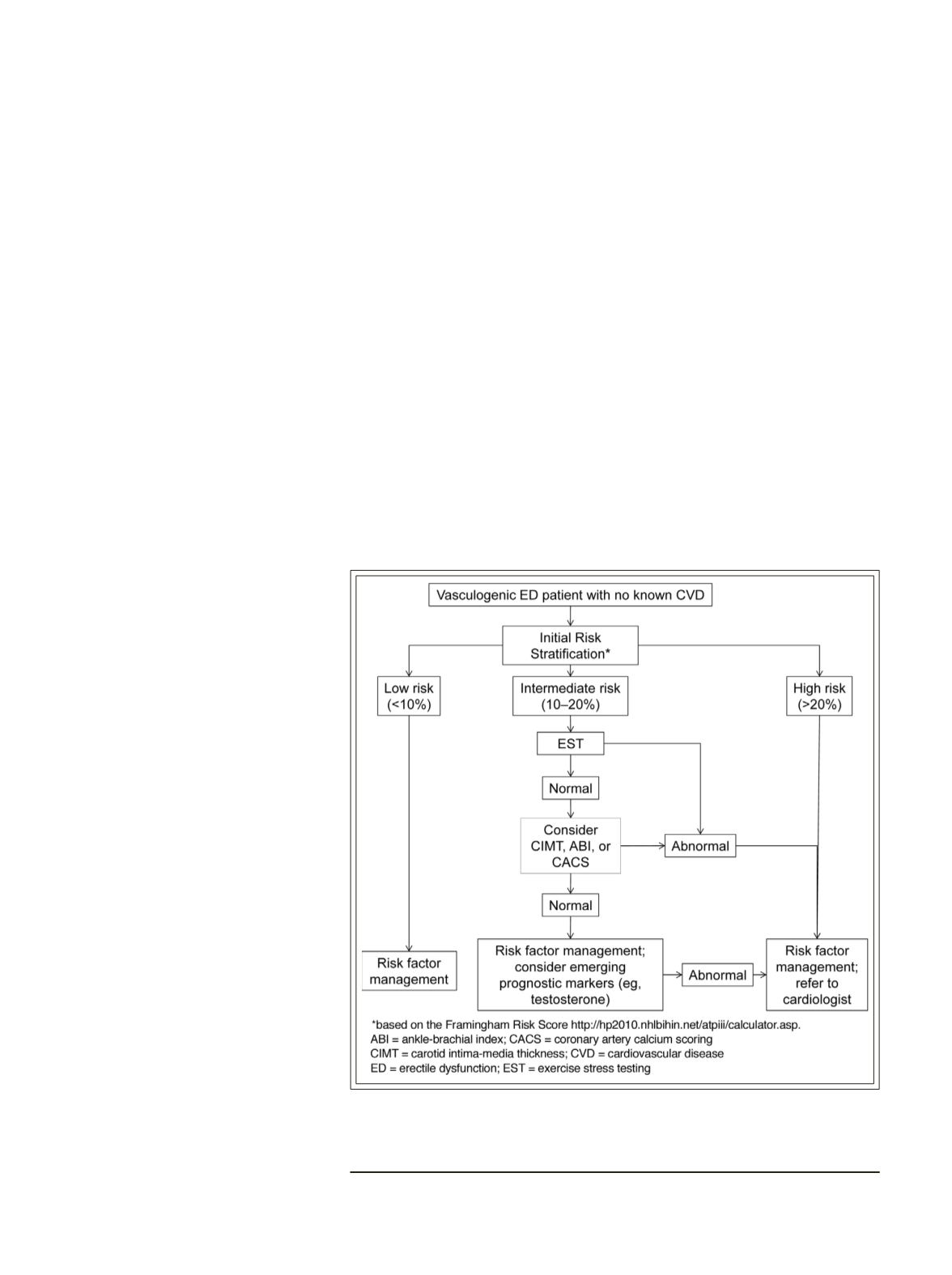
Figure 1.
Recommended evaluation and management of cardiovascular
risk in men with vasculogenic erectile dysfunction but no known CVD for
the primary care physician.
coronary artery calcium scoring
(CACS) to determine the extent of
subclinical atherosclerotic plaque
burden, Figure 1. Neither the
most appropriate order of testing
nor the prognostic superiority
of one test over another has
been established. Tests should
be selected based on clinical
judgment, availability, and
cost. All are considered a class
IIB where the benefit appears
to outweigh the risk and one
or another of the tests may
indicate plaque burden in an
asymptomatic intermediate risk
patient.
Exercise stress testing (EST):
i n c l u d i n g my o v i ew o r
echocardiographi c stress
testing
The 2010ACCF/AHAguidelines
recommend EST and CIMT
for noninvasive evaluation of
subclinical CVD in intermediate-
risk patients.
53
Although EST
does not detect non-flow-limiting
lesions, it detects silent, inducible
ischemia, thus providing further
understanding of CVD risk. Data
29
Erectile dysfunction in primary care: a focus on cardiometabolic risk evaluation and stratification for future
cardiovascular events


