©TheCanadian Journal ofUrology™: International Supplement, April 2014
prostatecancerpatients. Lateron,50%ofbonemetastatic
castration resistantprostatecancer (CRPC)patientswill
experienceoneormoreSREs.
30,31
In theZAregistration
trial, themeanannual incidenceof SREs in theplacebo
groupwas 1.47.
32
Thepresence of SREs is significantly
associatedwithworsesurvival,poorerquality-of-life in
CRPCpatients, anda significant cost for thehealthcare
system.
33,34
Pharmacologicalpreventionof SREs, Table3
Thebisphosphonatesclodronateandpamidronatewere
tested against placebo in three trials with palliative
endpoints, both failing to provide significant clinical
benefit, explainingwhy these drugs have never been
widelyprescribedbyurologists inmetastaticpatients.
Triweekly clodronate (intravenous (IV) 1500mg) has
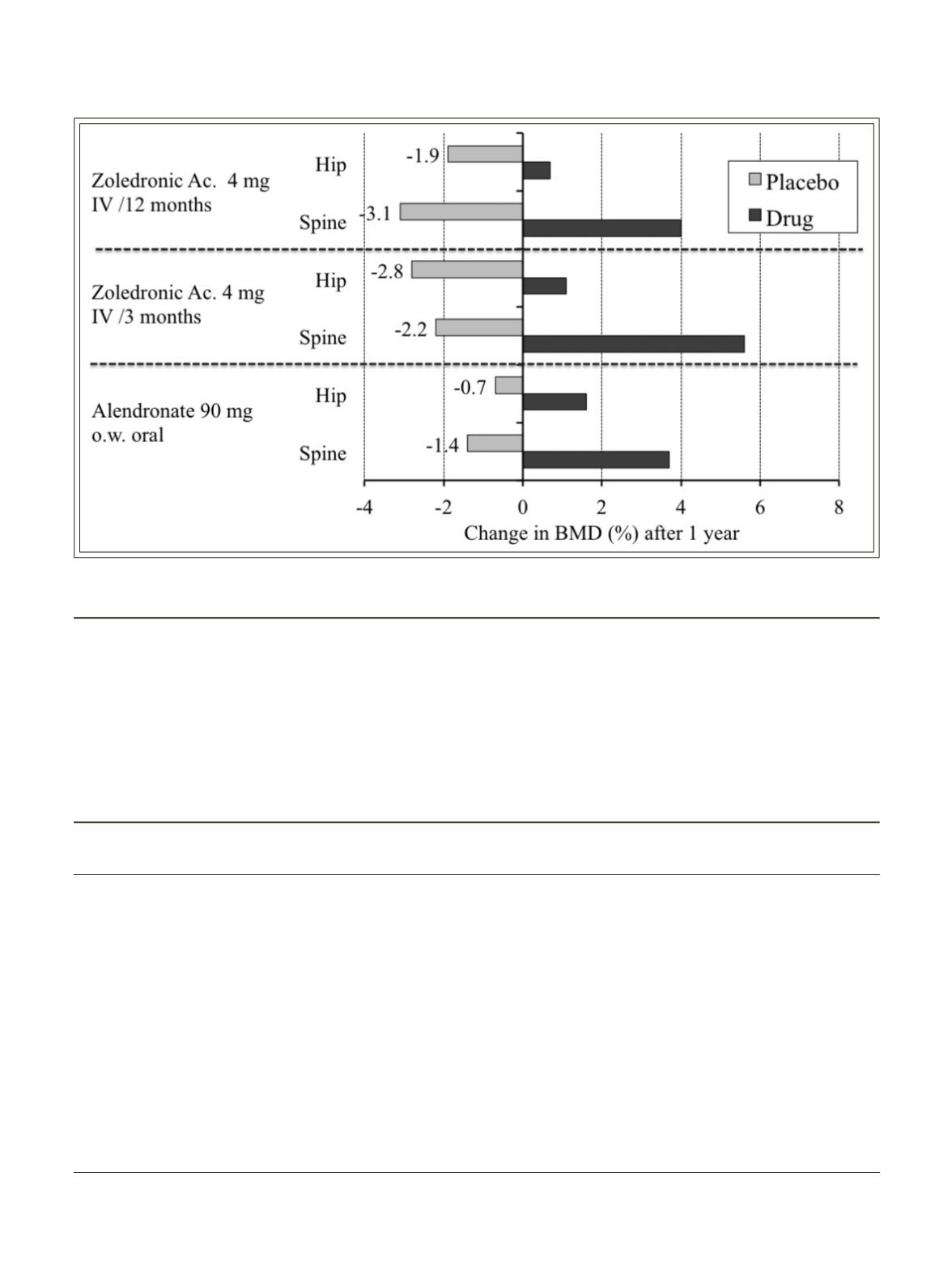
Figure 1.
Benefit of bisphosphonate of prevention of androgen deprivation therapy induced cancer treatment
inducedbone loss inprostate cancer patients.
TABLE 3.
Summary of studies evaluating bone targeted agents in the prevention of SRE in bonemetastatic
CRPCpatients
Drugs
Pamidronate
Zoledronate
Denosumab
versusplacebo
36
versusplacebo
32
versus zoledronate
31
Number of patients
320
422
1701
Studyduration
Fixed at 27weeks
Fixed at 24months
Event-driven,
maximum41months treatment
%patientswithSRE (p)
25versus 25 (NR)
38versus 49 (0.009)
36versus 41
Median time tofirst
Not tested
16.0versus 10.5;
20.7versus 17.1
on-studySRE (months)
p= 0.009
p= 0.0002non-inferiority,
0.008 superiority
Benefit on time tofirst
Not tested
HR= 0.64;
HR= 0.82;
and subsequent SREs
p= 0.002
p= 0.008
SRE= skeletal related event; CRPC= castration resistant prostate cancer;HR=hazard ratio
87
ButoescuANDTombal


